Document Type : Original article
Abstract
Background: Determining the exact location of mandibular foramen is an important factor prior to Inferior Alveolar Nerve (IAN) block injection. The aim of this study is to assess the position of Mandibular Foramen (MF) and its variations using Cone-Beam Computed Tomography (CBCT).
Methods: This study was conducted on CBCT images of 80 females and 80 males (18 to 68 years). The distance between the MF and the anterior border of ramus (A), inferior border of mandible (B), superior border of mandible (C), and occlusal plane was measured. Data were analyzed by the student t-test, bivariate correlation analysis, paired sample t-test, and Pearson’s correlation coefficient.
Results: The mean amount of A, B and C distances, and the mean distance from the occlusal plane to the center of MF were 13.76, 24.24, 12.32, and 7.59 mm, respectively, with no significant difference between the right and left sides (p>0.05). The mean B and C distances were significantly smaller in females than males (p<0.05). The mean size of the measured angle was 43.2°. Significant correlations were noted between aging and decreased A distance, and reduction in the angle between the contralateral premolars and MF (p<0.05).
Conclusion: Knowledge about the position of MF can enhance the surgical procedures in this region. Using a 21-25 mm needle would be associated with lower risk of needle fracture during IAN block injection. Also, needle insertion angle <45-degrees is optimal for the samples assessed in this study.
Keywords: Anatomies, Cone-beam computed tomography, Mandibular foramen
Introduction
The Inferior Alveolar Nerve (IAN) enters the mandibular ramus through the Mandibular Foramen (MF). The MF is located in the internal surface of the mandibular ramus, a few millimeters (mm) above the occlusal plane of molar teeth and approximately at the center point of the mandibular ramus close to the sigmoid notch. However, some anatomical variations exist in the position of MF in different individuals (1). To achieve a successful IAN block, the anesthetic agent should reach the MF. Insertion of the needle far from the MF prevents the access of anesthetic agent to IAN (2,3). Failure in IAN block and reinjection can lead to trismus, which causes patients’ discomfort and complicates the conduction of surgical procedures (4).
Long needles are recommended for IAN block (3). However, a study conducted on dry mandibles showed that short needles with 25 mm length can also be used for IAN block due to the position of the MF (1). Using a short needle decreases the risk of needle fracture during IAN block injection. Dentofacial deformities such as retrognathism and prognathism are common. Sagittal split ramus osteotomy is performed to correct such deformities (5). Correct determination of the anatomical location of MF is imperative for an optimal incision line and fracture line in the mandibular ramus and to prevent IAN damage and related complications in this surgical procedure.
Considering all the above, knowledge about the position of MF in each population is necessary. Thus, this study aimed to assess the position of MF in an Iranian subpopulation using Cone-Beam Computed Tomography (CBCT).
Materials and Methods
This descriptive cross-sectional study was conducted on 160 CBCT images of the mandible retrieved from the archives of the school of dentistry of Shahid Beheshti University of Medical Sciences. The study was approved by the ethics committee of the mentioned university (IR.SBMU.RIDS.REC.1396.593). CBCT scans of 80 males and 80 females with a mean age of 18 to 68 years were selected by convenience sampling. All CBCT scans had been taken with NewTom VGI CBCT scanner (Verona, Italy). The minimum sample size was calculated to be 65 according to previous studies (5,6) assuming α=0.05, 95% confidence interval, standard deviation of 4.1 mm, and accuracy of 1 mm.
Inclusion and exclusion criteria
The inclusion criteria were CBCT images of the mandible visualizing both mandibular rami, age range of 18-68 years, and complete eruption of canine and molar teeth. The exclusion criteria were mandibular asymmetry, images with artifacts, presence of pathological lesions, poor or no visualization of MF at one or both sides on images, and missing of molars and/or canine teeth.
CBCT assessments
To determine the head position, the occlusal plane alignment was evaluated using the NNT Viewer software (version 8.0), such that the anterior border of the MF had to be at the level of the line tangent to the occlusal surface of the mandibular second molar (6).
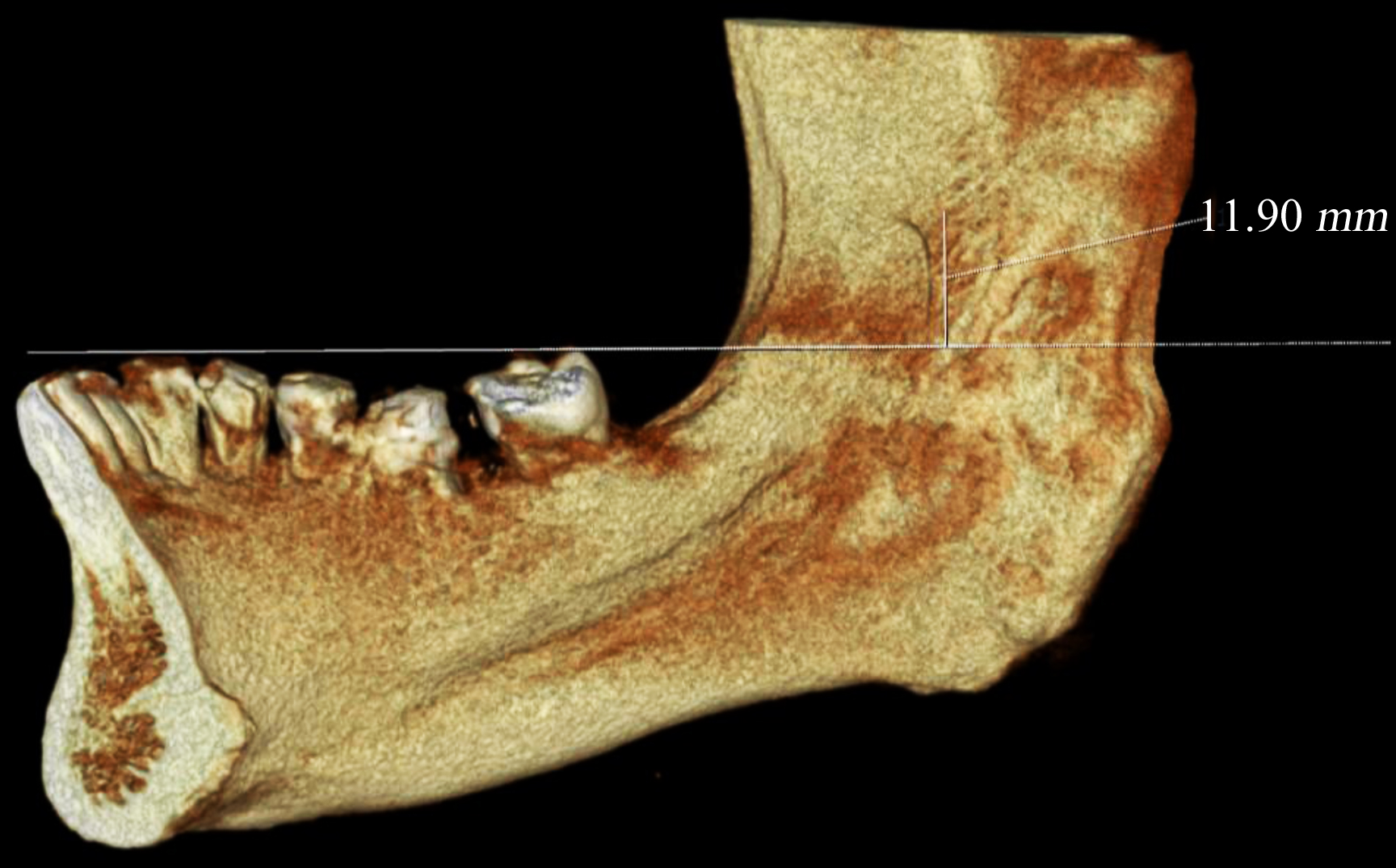
To determine the position of MF in the mandibular ramus, four distances were measured on CBCT images in NNT Viewer software and reported in millimeters. The distances and their definitions were as follows (Figure 1):
Distance A: Distance (Mean±SD) between the anterior border of MF and the cortex of the anterior border of mandibular ramus.
Distance B: Distance (Mean±SD) between the inferior border of MF and cortex of the inferior border of mandibular ramus.
Distance C: Distance (Mean±SD) between the superior border of MF and cortex of the superior border of mandibular ramus.
The distance between the occlusal plane and the center of MF was also measured on CBCT scans. Prior to the measurements, the 3D position of the mandible was standardized. For this purpose, the occlusal reference plane was drawn from the tip of canine and mesiobuccal cusps of mandibular first and second molars parallel to the horizon. The distance between the midpoint of the MF and the occlusal plane was then measured (6) (Figure 2).
Also, to determine the correct angle of needle insertion for an IAN block, the angle formed between the line connecting the contralateral premolars and the center of MF, and the line connecting the right and left premolars was measured on 3D CBCT scans (7) (Figure 3). The abovementioned distances were measured by the ruler feature of NNT Viewer software and reported in mm. The aforementioned angle was measured by the caliper feature of the software and reported in degrees. The age and gender of the patients were also recorded from patients’ records available in the archives. Data (Mean± SD, Min, Max) were analyzed using IBM SPSS STATISTICS 24 (IBM Corp., Armonk, New York, USA) by Student t-test, bivariate correlation analysis, paired sample t-test, and Pearson’s correlation coefficient.
Results
A total of 160 CBCT scans of 80 males and 80 females with a mean age of 36.45 years were evaluated. The mean age was 38.25 years for males and 33.23 years for females. The mean amounts of A, B and C distances, and the mean distance from the occlusal plane to the center of MF were 13.76±2.21, 24.24±3.57, 12.32±3.11 and 7.59±3.14 mm, respectively. Table 1 presents the mean amounts of A, B and C distances, and the mean distance from the occlusal plane to the center of MF in the right and left sides. As shown, no significant difference was noted between the right and left sides in any of the measured distances (p>0.05). Table 2 presents the mean amounts of A, B and C distances, and the mean distance from the occlusal plane to the center of MF in males and females.
Table 1. Mean amounts of A, B and C distances, and the mean distance from the occlusal plane to the center of MF in the right and left sides
|
Measurement |
Side |
Number |
Mean |
SD |
Minimum |
Maximum |
p-value |
|
|
Right |
160 |
13.56 |
2.47 |
7.5 |
20.4 |
|
|
A |
|
|
|
|
|
|
0.085 |
|
|
Left |
160 |
13.96 |
2.43 |
8.1 |
19.8 |
|
|
|
Right |
160 |
24.47 |
3.73 |
14 |
32.6 |
|
|
B |
|
|
|
|
|
|
0.098 |
|
|
Left |
160 |
24.01 |
4.21 |
3.9 |
36 |
|
|
|
Right |
160 |
Table 2. Mean amounts of A, B and C distances, and the mean distance from the occlusal plane to the center of MF in males and females
|
Measurement |
Gender |
Number |
Mean |
SD |
Minimum |
Maximum |
p-value |
|
|
Female |
80 |
13.65 |
2.39 |
8.55 |
19.20 |
|
|
A |
|
|
|
|
|
|
0.544 |
|
|
Male |
80 |
13.87 |
2.02 |
7.95 |
18.90 |
|
|
|
Female |
80 |
23.06 |
2.54 |
17 |
28.05 |
|
|
B |
|
|
|
|
|
|
0.032 |
|
|
Male |
80 |
25.41 |
4.05 |
12.75 |
33.45 |
|
|
|
Female |
80 |
11.87 |
2.67 |
6 |
17.85 |
|
|
C |
|
|
|
|
|
|
0.034 |
|
|
Male |
80 |
12.78 |
3.45 |
6.15 |
22.15 |
|
|
|
Female |
80 |
7.26 |
2.83 |
1.05 |
15.35 |
|
|
Occlusal plane |
|
|
|
|
|
|
0.197 |
|
|
Male |
80 |
7.91 |
3.41 |
1 |
16.55 |
|
Table 3. Mean size of the angle in the right and left sides, and in males and females
|
Parameter |
Category |
Number |
Mean |
SD |
Minimum |
Maximum |
p-value |
|
|
Right |
160 |
5.43 |
2.57 |
40 |
3.49 |
|
|
Side |
|
|
|
|
|
|
0.095 |
|
|
Left |
160 |
1.43 |
2.48 |
4.40 |
5.49 |
|
|
|
Male |
160 |
43.7 |
2.67 |
40.4 |
49.5 |
|
|
Gender |
|
|
|
|
|
|
0.089 |
|
|
Female |
160 |
43 |
2.38 |
40 |
49.3 |
|
As shown, the mean B (p=0.032) and C (p=0.034) distances were significantly smaller in females than males. The mean angle formed between the line connecting the contralateral premolars to the center of MF and the line connecting the right and left premolars was 43.2±3.22 degrees, irrespective of age and laterality. Table 3 presents the mean size of this angle in the right and left sides and in males and females. As shown, no significant difference was noted in this regard between the right and left sides (p=0.095) or males and females (p=0.089).
Table 4 presents the results of Pearson’s correlation coefficient for the correlation of each parameter with aging. As shown, aging had a significant correlation only with the A distance (Pearson’s correlation=-0.161, p=0.041) and the measured angle (Pearson’s correlation=-0.172, p=0.044).
Table 4. Results of Pearson’s correlation coefficient for the correlation of each parameter with age
|
|
A |
B |
C |
Occlusal plane |
Angle |
|
p-value |
0.041 |
0.053 |
0.637 |
0.648 |
0.043 |
|
Pearson’s correlation coefficient |
-0.161 |
0.153 |
0.038 |
-0.036 |
-0.172 |
Discussion
Mandibular foramen is an important anatomical landmark containing the inferior alveolar nerve. A precise detection of this anatomic landmark is prerequisite prior to most mandibular cosmetic orthognathic surgeries, osteotomies, surgical excision of pathologies and IAN block injection. The success of IAN block is lower than the maxillary blocks due to different reasons such as the penetration depth of the needle into the soft tissue, accessory innervations, and anatomical variations of the position of MF (3-8). Thus, correct insertion of the needle close to the MF is imperative. Injection of anesthetic agent posterior to the MF and in the posterior ramus can lead to facial nerve paralysis or damage to the parotid gland (9,10). This study assessed the position of MF in an Iranian subpopulation using CBCT. CBCT provides three-dimensional assessment of maxillofacial skeleton and offers higher spatial resolution with lower radiation exposure in contrast to conventional CT. In this study, the anteroposterior position of MF was determined by measuring the distance of MF to anterior border of ramus, since it can serve as a reference for the length of needle insertion for an IAN block (11). This distance was found to be averagely 13.76 mm with no significant difference between the right and left sides, or males and females in our study population. This distance, in addition to approximately 7 mm thickness of soft tissue (1), indicates that 20.76 mm distance averagely exists between the point of needle insertion and MF. Thus, injection needles with 21 to 25 mm length can be used for IAN block injections. This value was measured to be 13.76 mm in the present study, which was close to the value reported by da Silva Braga et al (12) (11.81 mm) in a Brazilian population but lower than the value reported by Kang et al (6) in a Korean population (22.9 mm). Both of the aforementioned studies made the measurements on CBCT scans, similar to our methodology.
The present results showed a significant correlation between age and the distance of MF to anterior border of ramus; however, this correlation was not strong, and may be due to resorption of the anterior ramus and absorption in the posterior ramus at a very slow rate, compared with the pace of aging, in older patients.
In this study, the distance between the occlusal plane and MF was also measured because it can serve as a reference for needle insertion in IAN block injections. Feuerstein et al (13) used the mandibular plane as a fixed clinical reference in all ages to determine the position of MF. The significance of locating the MF by using the occlusal plane irrespective of the experience and skills of the clinician is undeniable (13). This distance was measured to be 7.59 mm in our Iranian population with no significant difference between the right and left sides or males and females. This value was higher than the value measured by Kang et al (6) in their study on a Korean population (3.8 mm) and the value reported by Lima et al (14) in a Brazilian population (5.57 mm). Hwang et al (15) reported that the position of MF relative to the occlusal plane changed with age such that the MF was below the occlusal line in children while it was 4.16 mm above the occlusal line in adults. This association was not significant in the present study.
The mean distances between the MF and the inferior border of mandible and superior border of mandible were significantly smaller in females than males in the present study. The same results were reported by Kane et al (16) and Lo et al (17). This difference can be attributed to weaker muscle structures in females, which leads to lower growth of the mandibular ramus and subsequent impact on the position of MF (18).
The distance between the MF and inferior border of mandible and superior border of mandible had no significant correlation with age in the present study. Also, the distance between the MF and the anterior border of ramus, inferior border of mandible and superior border of mandible and occlusal plane-MF distances were not significantly different in the right and left sides, indicating the presence of symmetry in position of MF in the right and left sides in our Iranian population. Similar results were reported by Valente et al (19,20).
Moreover, the angle formed between the line connecting the contralateral premolars to the center of MF and the line connecting the right and left premolars was measured to be 43.1 degrees in the left and 43.5 degrees in the right side, respectively, in the present study, which were almost similar to the values reported by Blacher et al (7). In the study by Kang et al (6), the angle formed between the line connecting the contralateral premolars and the contact point of second premolar and first molar of the mandible of the other side, and the line connecting the MF and sagittal plane was measured to be 51.2 and 56.5 degrees. Differences in values reported by the two studies in this respect can be due to the use of a different reference point by Kang et al (6) for the measurements. Needle insertion with an angulation <45 degrees relative to the line connecting the right and left premolars increases the chance of adequate approximation of needle tip to the MF in the Iranian population (21). However, clinical assessment of the exact position of MF would increase the odds of a successful IAN block because the size of this angle in the Iranian subpopulation was different from the value reported by Blacher et al (7) in an American population.
In the present study, a significant correlation existed between age and the abovementioned angle. However, this correlation was not strong. Also, this angle was not significantly different in the right and left sides, or between males and females, which was in line with the results of Blacher et al (7).
This study had some limitations. The distance between the posterior border of mandible and MF was also intended to be measured. However, it was not possible to measure this distance due to small field of view of images and no visualization of the posterior border of ramus on most CBCT images (22-24). Future studies are required to assess the position of MF in patients with class I, II and III malocclusions.
Conclusion
Knowledge about the mean amounts of distance between the MF and the anterior border of ramus, inferior border of mandible and superior border of mandible can aid in conduction of surgical procedures in this region. Using a 21-25 mm needle would be associated with lower risk of needle fracture during IAN block injection. Also, needle insertion angle <45-degrees is optimal according to the obtained results.
Availability of the data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical approval
The study was approved by the ethics committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.RIDS.REC.1396.593). The study protocol was approved by the institutional review board of Shahid Beheshti University of Medical Sciences.
Funding
This research received no specific grant from any funding agencies.
Consent for publication
All authors consent to publication of this manuscript.
Conflict of Interest
The authors declare that they have no conflict of interests.