Document Type : Original article
Abstract
Background: Management of patients with Gastrointestinal Bleeding (GIB) based on chronicity and severity of it can vary from outpatient medical therapy to intensive caring in life-threatening cases. Initial clinical management decision in patients presenting to emergency department with acute GIB is often based on identifying high- and low-risk patients. Patients with high risks of adverse outcomes, such as death or re-bleeding, are more likely to benefit from early, aggressive management, whereas patients with lower risks may be considered for early hospital discharge or even outpatient management. Serum lactate level is generally an indicator of the overall adequacy of peripheral oxygenation. In severe cases of acute GIB, the hemodynamic of the patients disturbs. In this study, we are evaluating whether higher serum lactate level is potentially a biomarker for predicting the future need for special management considerations.
Methods: 168 patients with confirmed acute GIB have entered this study. The serum lactate level of participants was measured and documented as well as their demographic data and their medical history. The participants’ need for ICU admission, blood transfusion, emergent endoscopy, and mortality rate were documented and assessed prospectively.
Results: Patients with higher levels of serum lactate levels were more admitted to the intensive care unit in the upcoming days. Anticoagulant use and abdominal pain prevalence were also significantly different in the study groups (p>0.05). Other assessments were not statistically significant.
Conclusion: Higher levels of serum lactate predict a higher probability of ICU admission in patients with acute GIB.
Keywords: Biomarkers, Gastrointestinal hemorrhage, Intensive care units, Lactates
Introduction
Gastrointestinal (GI) bleeding, including Lower (LGIB) and Upper (UGIB) GI bleeding, is a life-threatening condition that has long been under attention due to considerable mortality and fatality. Significant clinical and economic burden imposed on health care systems by LGIB and UGIB and the need for hospitalization for immediate diagnosis and treatment in many cases are important factors in managing health care costs in different countries (1). In some studies, the mortality rate of GI bleeding has been reported to be between 3 and 14%. Also, it has been reported that around 45 to 60% of cases of hospitalization due to acute GI bleeding are due to Peptic Ulcers Disease (PUD) (2).
The annual incidence of GI bleeding in the last decade has been approximately 90-108 per 100,000 population, including approximately 300,000 of hospitalizations per year. The main reason of bleeding in most patients is peptic ulcer, which is associated with noteworthy mortality (3-14%) and imposes high economic burden on the health care system (3).
As it is important to rapidly diagnose and treat high-risk patients, various risk assessment systems have been designed to timely identify such patients. Developed scoring systems are often based on clinical, laboratory, and endoscopic findings. However, due to the fact that endoscopic findings are often not available upon initial assessments, the assessment systems that are based on clinical and laboratory data seem to be more efficient for initial assessment and treatment of patients (4).
Blood lactate level has been shown to predict disease severity and mortality risk in patients with sepsis. In the human body, lactate is produced by the action of the Lactate Dehydrogenase (LDH) enzyme which reduces pyruvate. Under normal physiological conditions, no reaction in the body results in the production of lactate, and actually this pathway accounts for only one-tenth of the total pyruvate metabolism (5). In a normal individual, the total daily production of lactate is 1500 mM, thus blood lactate level is naturally less than 2 mM/L. Nevertheless, in critical conditions, pyruvate rapidly accumulates in the body, and enzymatic reactions are shifted toward lactate production. As a result, intracellular lactate and subsequently its level in the blood rise (6).
Numerous studies have examined the predictive value of blood lactate level for the outcomes of acute GI Bleeding (7). A few studies have been conducted to assess serum lactate level in patients with acute GI bleeding referred to hospitals in Iran, so there is a need to address this issue. In the present study, we evaluated blood lactate level and its association with important clinical outcomes in patients with GI bleeding.
Materials and Methods
This was a cohort study performed on patients with acute GI bleeding referred to the Loghman Hakim Hospital in Tehran. Informed written consent was obtained from the patients before including them in the study. After measuring blood lactate levels, the patients were categorized into two groups of normal and high lactate level. The normal range of serum lactate was considered 4.5 to 18 mmol/L, and those with levels equal or higher than 18 mmol/L were regarded to have elevated lactate levels.
Patients’ information including age, sex, serum lactate level, need for blood transfusion, need for hospitalization in the Intensive Care Unit (ICU), and need for emergency endoscopy were recorded. Other collected data consisted of history of taking NSAID, corticosteroids, and anticoagulants, smoking, alcohol consumption, signs of hematemesis, hematochezia, and melena, the presence of abdominal pain, as well as vital signs (blood pressure, heart rate), the patient’s consciousness level and tilt test, along with laboratory parameters including Cr, Plt, INR, Hb, and serum lactate.
Patients were screened for inclusion and exclusion criteria. Inclusion criteria were the diagnosis of GI bleeding and age of >18 years. Exclusion criteria were unwillingness to participate and incomplete medical records. We also recorded potentially confounding variables (using specific drugs, smoking, and alcohol consumption) and considered their effects in the statistical analyses.
Statistical analysis of the data was performed employing inferential statistics including independent t-test (or its equivalent in case of non-normally distributed data), Chi-square (or Fisher’s exact test in case of non-normal distribution), and multivariate logistic regression. Analyses were conducted in IBM SPSS statistical software (Version 22) (8). Confounding variables were considered as smoking, alcohol consumption, and using specific drugs according to the study of Shrestha et al (9). Informed consent was obtained from the patients before using their medical data. All the patients received standard treatment, and none were denied standard treatment due to participation in the study. Also, no additional costs were imposed on the participants.
Results
In this study, patients with acute GI bleeding were divided into two groups (n=84 per group) of elevated and normal serum lactate level. Overall, 107 (63.7%) of the patients were male (56 participants in the elevated serum lactate and 51 participants in the normal serum lactate group). The mean ages of the participants in the elevated and normal serum lactate levels were 66.71±16.86 and 61.32±19.29 years, respectively. The comparisons of different variables between the studied groups have been shown in table 1. According to Fisher’s exact test, the mean age of the participants was higher in the elevated serum lactate compared with normal serum lactate group (p=0.055 and t=1.929). There were no significant differences between the two groups in terms of gender, smoking, alcohol consumption, hematemesis, melena, hematochezia, consciousness, tilt, heart rate, and using corticosteroid or NSAID. However, there were significant differences regarding anticoagulant usage (p=0.004), abdominal pain (p=0.043), systolic blood pressure(p=0.021) and ICU admission (p=0.045). Accordingly, a higher ratio of patients with elevated serum lactate (20.2%) had a history of anticoagulant usage than patients with normal serum lactate (4.8%). On the other hand, more patients with normal serum lactate had a history of abdominal pain than those with elevated serum lactate (52.4% vs. 35.7%).
There was also a significant difference between the two groups regarding the mean value of systolic blood pressure, and a higher value was recorded in patients with normal lactate level (p=0.021). Considering the laboratory parameters (Plt, INR, HB, Cr), there were no significant differences between the two groups (Table 2).
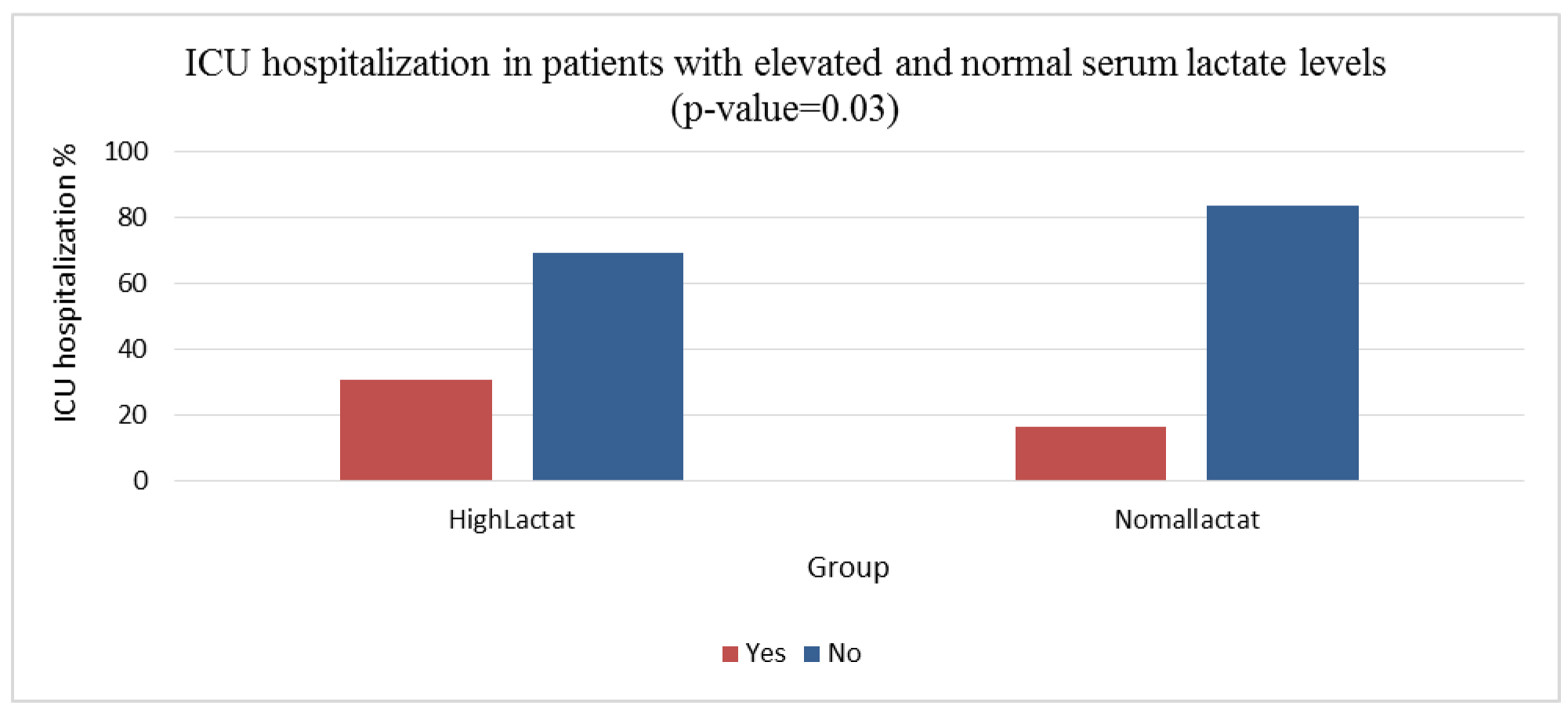
Regarding the needs for blood transfusion, emergency endoscopy, and ICU admission, as well as mortality, there was a significant difference between the studied groups only for hospitalization in the ICU (p=0.045, Table 3). In this regard, 31% of the patients with elevated lactate and 16.7% of the patients with normal lactate needed to be admitted to the ICU (Figure 1).
Table 1. Distribution of the demographic and clinical variables between the patients with elevated and normal serum lactate level
|
p-value |
Low lactate population |
High lactate population |
Total population |
Population characteristics |
|
1.000 |
14 (16.7%) |
13 (15.5%) |
27 (16.1%) |
Smoking |
|
0.620 |
3 (3.6%) |
1 (1.2%) |
4 (2.4%) |
Alcohol |
|
0.355 |
46 (54.8%) |
39 (46.4%) |
85 (50.6%) |
NSAIDs |
|
0.620 |
1 (1.2%) |
3 (3.6%) |
4 (2.4%) |
Corticosteroids |
|
0.004* |
4 (4.8%) |
17 (20.2%) |
21 (12.5%) |
Anticoagulants |
|
0.264 |
15 (17.9%) |
22 (26.2%) |
37 (22.0%) |
Tilt |
|
0.134 |
9 (10.7%) |
17 (20.2%) |
26 (15.5%) |
Mental situation |
|
0.271 |
46 (54.8%) |
54 (64.3%) |
100 (59.5%) |
Hematemesis |
|
0.134 |
17 (20.2%) |
9 (10.7%) |
26 (15.5%) |
Hematochezia |
|
0.209 |
39 (46.4%) |
30 (35.7%) |
69 (41.1%) |
Melena |
|
0.043* |
44 (52.4%) |
30 (35.7%) |
74 (44.0%) |
Abdominal pain |
Table 2. Laboratory parameters in the patients with elevated and normal serum lactate levels
|
|
High lactate |
Normal lactate |
Total |
p-valuea |
|||
|
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
|
|
Age |
66.7 |
16.9 |
61.3 |
19.3 |
64.0 |
18.3 |
0.091 |
|
HR |
92.5 |
18.5 |
87.9 |
15.2 |
90.2 |
17.0 |
0.041 |
|
SBP |
107.00 |
23.68 |
115.36 |
22.88 |
111.18 |
23.59 |
0.009 |
|
INR |
1.91 |
2.26 |
1.50 |
1.99 |
1.70 |
2.13 |
0.006 |
|
Hb |
11.3 |
12.2 |
10.3 |
3.2 |
10.8 |
8.9 |
0.726 |
|
Plt |
221.7 |
129.9 |
225.8 |
98.1 |
223.7 |
114.8 |
0.301 |
|
Cr |
1.7 |
1.1 |
1.8 |
1.5 |
1.8 |
1.3 |
0.797 |
a: Mann-Whitney U test.
Table 3. Distribution of the requirements for blood transfusion, emergency endoscopy, and ICU admission, as well as mortality in patients with elevated and normal serum lactate level
|
p-value |
Low lactate population |
High lactate population |
Total population |
Population characteristics |
|
1.000 |
43 (51.2%) |
43 (51.2%) |
86 (51.2%) |
Blood transfusion |
|
1.000 |
26 (31.0%) |
27 (32.1%) |
53 (31.5%) |
Endoscopy |
|
0.045* |
14 (16.7%) |
26 (31.0%) |
40 (23.8%) |
ICU admission |
|
0.820 |
10 (11.9%) |
12 (14.3%) |
22 (13.1%) |
Mortality |
Discussion
GI bleeding is one of the most common problems encountered in the internal medicine (10). GI bleeding is defined as any form of abnormal blood loss from GI tract from the mouth to the rectum and it is clinically divided into LGIB and UGIB (11,12). LGIB and UGIB can have different underlying causes. Generally, PUDs, varices, esophageal vascular abnormalities, and Mallory Weiss are among the most common etiologies of UGIB (12) while Fisher, Diverticula, hemorrhoids, and benign and malignant lesions of colon are also among common causes of LGIB (11). GI bleeding can be acute or chronic. The incidence of chronic GI bleeding increases with age and can lead to the loss of blood cells, particularly erythrocytes, resulting in anemia, which can be the primary sign of a prolonged GI bleeding (13). Severe acute GI bleeding may lead to hemodynamic instability, hypotension, tachycardia, and subsequently hemorrhagic shock or a condition mimicking a shock, a phenomenon that is considered as a medical emergency in patients with acute GI bleeding and is associated with a high mortality (14). In such cases and depending on the patient’s clinical condition, intensive care, ICU admission, blood transfusion, and emergency endoscopy may be required to cease bleeding. In conditions in which bleeding is severe and occurs over a short period, reduced tissue blood supply and hypoxia result in certain laboratory signs and clinical symptoms.
Different levels of care are required to manage patients with GI bleeding. Patients without risk factors, who experience limited bleeding due to benign and mild underlying causes may be treated on an outpatient basis as the bleeding may be self-limited. Studies show that most GI bleeding cases are self-limiting and resolve spontaneously over a limited period of time with either causing no specific clinical symptoms or presenting with nonspecific ones (15). On the other hand, some patients, especially those with acute and extensive GI bleeding, may need emergency procedures to survive and avoid subsequent outcomes.
For appropriate management of the patients referred to the ICU due to GI bleeding, it is of critical importance to precisely predict the clinical course of the disease. In fact, favorable prognosis and timely diagnostic and therapeutic measures can reduce mortality and GI bleeding complications, especially in case of the exacerbation of the patients’ clinical condition (16). In this regard, different scoring and classification systems have been developed based on laboratory, clinical, and endoscopic findings. Among these scoring and prognostic systems, those that are based on endoscopic findings have a more limited clinical application due to the unavailability of endoscopic findings at early stages. The GBS test is widely used by therapists as one of the prognostic parameters in this condition.
Lactic acid is a byproduct of anaerobic energy production in the body. In aerobic metabolism, which constitutes the body’s common metabolic pathway, required energy is provided by the breakdown of pyruvate molecules in the presence of oxygen. In the case of impaired tissue oxygenation due to any reason, anaerobic metabolism is activated. During this metabolic pathway, which can be carried out in most cells of the body, pyruvate molecule is reduced to lactate by the LDH enzyme. The produced lactate can be released into the extracellular space and enter the bloodstream via diffusion (17). Nowadays, serum lactate level can be measured via routine laboratory tests. Studies have shown that serum lactate level may be slightly different between arteries and veins. This may be explained by the fact that lactate during a reverse process is reduced to pyruvate by the liver, which leads to the reduction of serum lactate level upon its passage through the liver (18). Based on these evidences, serum lactate can be used as a general indicator of tissue oxygen (17-19). Serum lactate levels may be elevated in several physiological and pathological conditions. In pathological conditions (especially shock); however, serum lactate serves as a measure to screen the deterioration of tissue oxygenation.
Extensive acute GI bleeding can lead to hemodynamic instability and inadequate tissue oxygenation. Therefore, it can be stated that by increasing the severity of bleeding and reducing the circulation system’s ability to supply enough oxygen to tissues, lactate level rises in the blood (19). This phenomenon shows an association between reduced tissue oxygenation and the severity of bleeding. On the other hand, patients with more extensive bleeding are more likely to require intensive care, blood transfusion, volume replacement, and invasive procedures to stop bleeding more quickly. Thus, serum lactate seems to be a good biomarker to predict the patients’ need for these therapeutic measures.
In this prospective study, the needs of patients with normal and elevated (>18 mM/L) serum lactate for intensive care procedures were compared. In order to reduce bias, the effects of potentially confounding variables such as age, gender, history of drug consumption, smoking, and alcohol abuse, which were selected based on a study by Shrestha et al (9), were adjusted in statistical analyses.
According to our findings, there were no significant differences between patients with elevated and normal serum lactate levels in terms of gender distribution, smoking, and alcohol consumption. Considering three groups of drugs including anticoagulants, corticosteroids, and NSAIDs, our results indicated no differences between the two groups comparing the usage of corticosteroids and NSAIDs. However, patients with elevated serum lactate levels were found to have a significantly higher rate of using anticoagulants. According to previous studies (20-22), using anticoagulants increases the risk and severity of GI bleeding. On the other hand, tissue oxygenation is affected following GI bleeding, so this can explain the association between elevated blood lactate level and the usage of anticoagulants. Nevertheless, we found no association between NSAIDs consumption, which has been noted to increase the risk of GI bleeding in vulnerable individuals, and elevated blood lactate level in our study.
Among the studied clinical symptoms, melena, hematochezia, and hematemesis showed no association with blood lactate level which may be due to the effects of other underlying factors or because of our relatively small sample size. However, patients with abdominal pain revealed significantly lower blood lactate levels, indicating a significant association between these two parameters. We also observed a significant relationship between elevated blood lactate levels and the need for ICU admission, which was in parallel with the findings of the previous studies (23-25). Nonetheless, no significant relationship was found between elevated blood lactate level and need for neither packed red cell transfusion or emergency endoscopy. Elevated lactate level had also no correlation with the risk of mortality in patients with GI bleeding, which may be due to our relatively low sample size and the low power of exploited statistical procedures. Considering the discrepancies among the finding of different studies, including ours, it is advisable to conduct studies with larger sample sizes and use more powerful statistical tests such as regression models to appropriately control the effects of confounding factors.
Conclusion
According to our findings, elevated serum lactate level in the patients presenting with GI bleeding may indicate a higher probability for ICU admission and requirement for intensive health care.
Acknowledgements
This research was supported by the Luqman Hakim Hospital Research Center.