Document Type : Original article
Abstract
Background: Poor Ovarian Response (POR) to ovarian stimulation is a challenging factor in Assisted Reproduction Technology (ART). This study aimed to compare the efficacy of a conventional antagonist with high doses of gonadotropin protocol with double stimulation protocol in females with POR.
Methods: This randomized clinical trial study was conducted on 60 women aged >35 with PORS at the Avicenna Infertility Center, Tehran, Iran. The participants were randomly divided into 2 groups (n=30 /each). In group 1, from the second day of the menstrual cycle, gonadotropin started at a dose of 450-600 units. In group 2, the second day of the menstrual period began with Letrozole 5 mg every night and an oral tablet of Clomiphene citrate 50 mg every day, and from the fourth day started 150 units of gonadotrophin (Triptorelin, 0.2 mg).
Results: In this study, at the end of the follicular phase, there was a significant correlation between protocol type and the number of Germinal Vesicles (GV) (p=0.04). The mean number of oocytes retrieved was 2.76±1.9 in the conventional method and 3.23±2.1 in the double stimulation group (p=0.90). The number of fertilized oocytes was 31 in the conventional protocol and 25 in the double stimulation protocol. The mean number of pregnancies that led to the fetus was 1.38±1.3 in the conventional protocol and 0.96±0.9 in the double stimulation group (p=0.018).
Conclusion: The results of this study show that the embryos in the double-stimulation group were more capable of completing the pregnancy, and the double-stimulation group had a higher live birth rate.
Keywords: Gonadotropin, Infertility, Oocytes, Ovulation induction
Introduction
Even today, significant progress has been made in assisted reproductive methods to achieve better results. However, only about 33% of the fertility rates of these methods have been reported. Poor Ovarian Response (POR) is a limiting factor during stimulation for In Vitro Fertilization (IVF). Among women referred for IVF, 5-24% experience POR (1,2(.
Meanwhile, a significant percentage of women who undergo assisted reproductive treatments respond poorly to gonadotropin stimulation (1). Poor ovarian response in IVF treatment is one of the most challenging situations for patients and doctors. These patients, called POR, comprise about 9-24% of women who have undergone IVF treatment (2,3).
There are different protocols for inducing ovulation during IVF. In the conventional method, high doses of gonadotropins are used to stimulate the growth of ovarian follicles. In this protocol, high doses of gonadotropins are administered in the early follicular phase to retrieve oocytes when the follicles mature (4-7). This protocol helps to restore an increased number of high-quality oocytes and to create a receptive endometrium. On the other hand, over-aggressive ovarian stimulation may increase the risk of hormone-related disorders as well as the risk of jaundice (8,9). The success rate of IVF in this category of patients is lower and different in various studies. In a review study, the rate of pregnancy resulting from IVF in patients with POR was about 14.8% compared to 34.5% in patients with a normal response (4).
POR was first described in patients with peak estradiol levels below 300 pg/ml and reduced follicular response. These patients had a smaller number of oocytes and as a result, they had less embryo transfer. POR may be accompanied by loss of ovarian capacity.
Patients with POR have a lower fertility rate compared to “normal” responders. Many criteria have been used to identify poor responders. Among these criteria, the two criteria “the number of dominant follicles” or “the number of oocytes obtained after the standard dose of the ovarian stimulation protocol” are among the most important (5,6).
According to the European Society of Fertility and Embryology (ESHRE), patients who have at least two of the following criteria are identified as POR: (Bologna criteria)
1. Elderly women or any other risk factor for weak ovarian response (previous ovarian surgery history or history of chemotherapy)
2. Previous poor ovarian response (getting less than 4 oocytes in the previous cycle)
3. The abnormality of ovarian reserve tests (7)
So far, different treatment protocols with high doses of gonadotropin, along with different adjuvant treatments have been used to improve ovarian response and fertility in this group of patients.
Recently, methods such as mild ovarian stimulation in the cycle of gonadotropin-releasing hormone agonist (GnRH agonist) with a low dose of gonadotropin using oral drugs such as anti-estrogens or aromatase inhibitors have been used in the IVF cycle in POR patients, and acceptable results have been obtained. In POR patients over 37 years of age, mild ovarian stimulation has been associated with similar results and sometimes even a slightly higher fertility rate compared to old conventional stimulation methods (8).
Successful cases of obtaining mature oocytes and embryos that can be frozen by starting the stimulation in the luteal phase have been reported in patients who needed to preserve the embryo due to emergency reasons, including various types of cancer and the need for chemotherapy (9,10).
Choosing the appropriate treatment protocol in POR patients to obtain mature oocytes and embryos of good quality and transferable is one of the most challenging issues of infertility. On the other hand, if the ovaries fail to respond to cycle therapy, it is better to use alternative methods, including the use of donated oocyte, which is difficult for majority of the patients to accept.
Regarding the effect of progesterone level increase on the oocyte trigger day and before their maturation on the thickness and pattern of the endometrium, endometrial receptivity, pregnancy rate, live birth as well as its effect on the quality of the resulting oocyte and embryos in different studies, very contradictory results have been reported and also the relationship between progesterone level and estradiol, Follicle-Stimulating Hormone (FSH), and Luteinizing Hormone (LH) levels on the same day and the day of gonadotropin initiation, as well as with the dose of gonadotropins, cycle length and the type of gonadotropins used (FSH) alone or combined FSH, Human Menopausal Gonadotropin (HMG) is discussed (11-16).
In 2014, a dual stimulation protocol (Xangai) was introduced by Kwong et al (10). They suggested that luteal phase follicles can produce mature oocytes similar to the follicular phase. Therefore, they used ovarian stimulation in the luteal phase after the follicular phase stimulation. They achieved a significant improvement in the number of mature follicles and embryos in a short period. Different studies also demonstrated the effectiveness of dual stimulation protocol on ovarian stimulation in patients with POR (11,12). However, it has not yet been investigated if the dual stimulation protocol has the potential to outperform the high-dose gonadotropin protocol.
In this clinical trial study, the effectiveness of the double stimulation treatment protocol (stimulation in both follicular and luteal phases) with a low dose of gonadotropin combined with oral anti-estrogen (clomiphene) and aromatase inhibitor (letrozole) drugs with the antagonist protocol were compared with the high dose of gonadotropin that is routinely used in these patients. The results of the microinjection cycle including the number of oocytes obtained, the number of suitable embryos, and finally the pregnancy rate during the double stimulation cycle is more or even equal to the conventional antagonist cycle, considering the acceptance of this method in many patients. It is more and the number of drugs used and the cost of drugs is much lower, thus it can be a great help for these patients.
This study was aimed at comparing the number and quality of mature oocytes and embryos as well as the rate of fertility in two groups of females with POR who underwent one of two protocols for ovarian stimulation before Intracytoplasmic Sperm Injection (ICSI) (17,18).
Materials and Methods
Study population
In this randomized clinical trial study, 60 women with POR who were referred to the Avicenna Infertility Center, Tehran, Iran, from April 2018 to November 2018, were investigated.
The studied population was randomly selected, from the computer system that included 500 poor responder patients. The participants were randomly selected based on the statistical formula of the sample size. Based on this the files of 500 patients with poor ovarian response were reviewed and among them 60 patients who agreed to participate in the plan and met the criteria for entering the plan were selected to participate in the study.
These 60 patients were randomly studied in two groups.
The number of 60 patients placed in the POR group based on the Bologna criteria were included in the study and assigned to one of the A or B groups according to the computerized sorting form. Randomization is initially done without the involvement of the researcher and by someone outside the study.
And the formula was calculated. The females were randomly divided into two groups1 (n=30/each) [(group 1 (DS)=Double stimulation protocol and group 2 (AHDG)=Conventional high doses of gonadotropins antagonist protocol)].
Sample size
According to the pregnancy rate of 56% in Shanghai group patients (19) and 14.8% in POR patients based on the report of a review study conducted (4) to show the difference between the two groups with 95% confidence and 80% test power of the relationship:
N = 2(z1-a/2+z1-β)2 (p) (1-p)
(P1-p2)2
In this study, according to the criteria of the European Society for Human Reproduction and Embryology for POR, the participants were chosen. Based on the criteria, at least two of the following three features should be present in POR (13): Age over 40; history of fewer than 4 oocytes; abnormal ovarian reserve tests; previous ovary surgery; risk factors in weak ovary response.
In the current study, the females with BMI > 35, FSH > 25, endometriosis > grade 3, and those who had any contraindication for ovarian stimulation such as uncontrolled systemic diseases, severe male infertility factors according to World Health Organization criteria were excluded (4).
In addition, two treatment cycles from each of the 60 patients, comparing the number of retrieved and mature oocytes, embryos, fertilization rates, and giving births were analyzed and also determined and compared serum levels of progesterone, FSH, LH, and Estradiol before and after the protocol administration.
The relationship between the level of progesterone hormone on the trigger day and the thickness and pattern of the endometrium in the same phase as also its relationship with the number and quality of oocytes and embryos obtained in that phase were investigated
The effectiveness of the dose of gonadotropins, the number of days of receiving them, and their type on the level of FSH, LH, E2, and PR hormones on the trigger day were investigated.
The effectiveness of the dose of gonadotropins and the number of days of receiving gonadotropins and their type on the level of FSH, LH, E2, and PR hormones on the trigger day were investigated.
The participants of the first group received double stimulation protocol and the second group received conventional high doses of gonadotropins for ovarian hyperstimulation.
Group 1: Conventional high doses of gona-dotropins antagonist protocol (AHDG group)
In the present study, a baseline transvaginal ultrasound on the second day of the follicular phase checked the number of antral follicles, endometrial thickness, and ovarian state. Also, a baseline laboratory test for serum levels of progesterone, FSH, LH, and estradiol was performed.
The patients were prescribed in this group to receive the following medications during the follicular phase starting from the second day of the menstrual cycle: subcutaneous human menopausal gonadotropin (HMG, 450-600 IU. Darou Pakhsh. Pharmaceutical Co., Tehran, Iran). The follicles were monitored and after they became 14mm in size, daily use of GnRH antagonists was administered. After they reached 16mm, a trigger was performed using a single injection of recombinant HCG (HCGR, 250 µg, Pooyesh Darou Pharmaceutical Co., Tehran, Iran) subcutaneously. The oocytes were retrieved 36 to 48 hours after triggering.
Group 2: Double stimulation protocol (DS group)
The participants in the double stimulation group received an oral tablet of clomiphene citrate 50 mg (Iran hormone. Pharmaceutical Co., Tehran, Iran) every day and an oral tablet of letrozole 5 mg (Iran hormone. Pharmaceutical Co., Tehran, Iran., 2.5 mg) every night from the second day of the menstrual cycle.They were treated with gonadotropins (Triptorelin, 0. 3 mg. Homa Pharmed. Pharmaceutical. Co., Tehran, Iran) after day 4 of the menstrual cycle. The rest of the protocol was carried out similarly to the first group. In this group, a second stimulation was performed 5 days after oocytes were retrieved. The second stimulation was completely similar to the primary stimulation.
Primary and secondary outcomes
Primary outcomes included
1- The number of oocytes obtained, periods of measurement: measuring the number of follicles at the beginning of the menstrual cycle and after taking ovulation stimulation drugs. The variable was measured by an ultrasound device.
2- Checking the number and quality of obtained embryos, periods of measurement: in the follicular and luteal phase, and the variable was measured by an ultrasound device.
3- Measurement of serum levels of Progesterone hormones, measurement periods: on the day of gonadotropin initiation and the trigger day with Deca ampoule in the follicular and luteal phase. The variable was measured by the ELISA method.
4- Measurement of serum level of hormone E2, measurement periods: on the day of gonadotropin initiation and the trigger day with Deca ampoule in the follicular and luteal phase. The variable was measured by the ELISA method.
5- Measurement of the serum level of LH hormone, measurement periods: on the day of gonadotropin initiation and the trigger day with Deca ampoule in the follicular and luteal phase. The variable was measured by the ELISA method.
5- Measurement of FSH serum level, measurement periods: on the gonadotropin initiation and the trigger day with Deca ampoule in the follicular and luteal phase. The variable was measured by the ELISA method.
7- The quality of the obtained oocyte, measurement periods: at the beginning of the menstrual cycle and after taking ovulation stimulation drugs. The variable was measured by an ultrasound device.
Table 1. The baseline characteristics of the patients in two study groups
|
|
Group1 (AHDG) |
Group2 (DS) |
p-value |
|
Age |
37.14±5.3 |
37.11±4.5 |
0.321 |
|
BMI |
24.99±2.4 |
25.05±4.0 |
0.244 |
|
FSH |
8.57±4.8 |
11.87±6.1 |
0.276 |
|
LH |
9.28±16.6 |
10.22±15.2 |
0.767 |
|
Estradiol |
68.25±48.2 |
48.13±21.7 |
0.014 |
|
AMH |
1.71±4.0 |
0.48±0.5 |
0.022 |
|
First transfer experience n (%) |
16(76.21%) |
16(61.5%) |
0.262 |
|
Primary infertility n (%) |
13(61.9%) |
21(80.76%) |
0.683 |
|
Years of infertility |
3.51±4.0 |
2.36±1.9 |
0.018 |
Note: AHDG: Antagonist with a High Dose of Gonadotropin, DS: Double Stimulation, BMI: Body Mass Index, FSH: Follicular Stimulating Hormone, LH: Luteinizing Hormone, AMH: Anti-Mullerian Hormone, Chi-square test.
Table 2. Comparison of laboratory findings between the participants with conventional and double stimulation protocol
|
|
Group1 (N=21) |
Group2 (N=26) |
p-value |
|
Oocytes |
2.76±1.9 |
3.23±2.1 |
0.804 |
|
GVs |
0.19±0.5 |
0.30±0.5 |
0.224 |
|
MI oocytes |
0.61±0.9 |
0.57±1.0 |
0.774 |
|
MII oocytes |
1.95±1.5 |
2.34±1.6 |
0.946 |
|
Fertilized oocytes |
1.38 ± 1.3 |
0.96±0.9 |
0.015 |
|
Blastocysts |
0.23±0.5 |
0.38±0.7 |
0.175 |
|
Giving birth |
0.04±0.2 |
0.15±0.3 |
0.018 |
|
Progesterone |
1.74±3.5 |
8.37±1.2 |
0.0078 |
|
Estrogen |
994.00±556.5 |
404.20±298.9 |
0.891 |
Note: AHDG: antagonist with a high dose of gonadotropin, DS: Double stimulation, BMI: body mass index, FSH: follicular stimulating hormone, LH: luteinizing hormone. Chi-square test
Secondary outcomes:
The rate of successful pregnancy and birth, measurement periods: after 9 months, and the variable is measured by the number of successful pregnancies and live births.
Ethical considerations
This study protocol was approved by the Tehran University of Medical Sciences (code: IR.ACECR.Avicenna.REC.1396.17) and has been documented in IRCTC.ir. All the participants received thorough information about the study. A written informed consent was received from each participant. Registration ID in IRCT: IRCT20180219038792N1, Approval date: 2019-01-02
Statistical analysis
The statistical analyses were performed using SPSS software version 19.0 (IBM Corp., Armonk, N.Y., USA). The student t-test was used for analysis to compare mean values and the chi-squared test (χ2) to compare the categorical variables. p-values < 0.05 were considered as significant.
Results
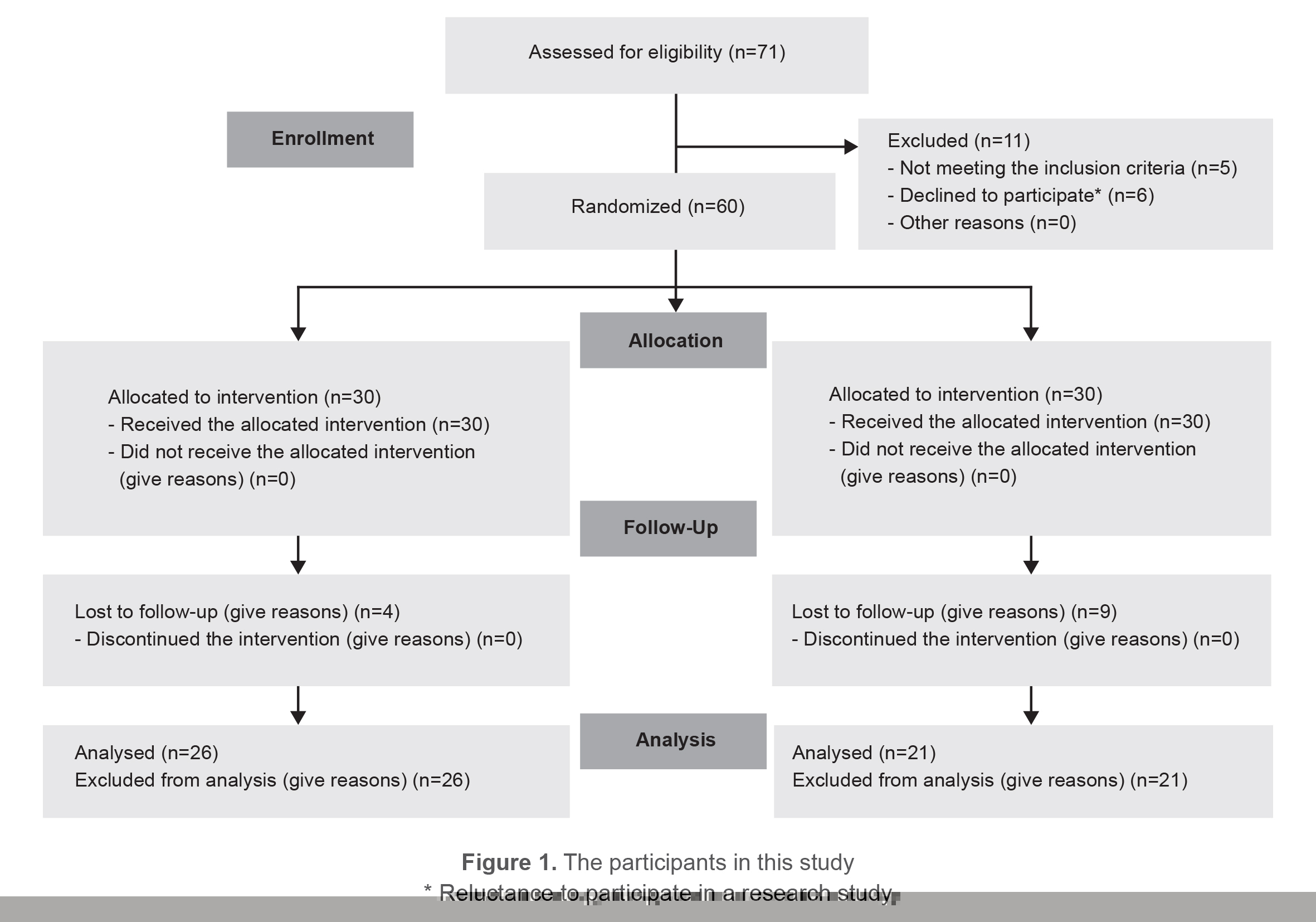
Initially, 60 women were enrolled in the study. 6 participants were excluded due to not meeting the inclusion criteria and 8 declined to participate. The remaining participants were randomly assigned to the intervention and control groups (n=30/each) Figure 1 show the graph of participants in this study. From the control group, 21 cases were excluded, and from 26 cases in the intervention group, the following were excluded: Of 60 patients, 21 in the antagonist with high doses of gonadotropin group and 26 in the double stimulation group completed the study. The baseline characteristics of each group are demonstrated in table 1. The mean results of the two groups did not differ significantly.
At the end of the follicular phase, in the conventional treatment group, two females had 1 Germinal Vesicle (GV) and one had 2 GVs in the vaginal ultrasonography. In the double stimulation group, 4 females had 1 GV, one of them had 2 GVs at first stimulation, and two had 1 GV at the end of the second stimulation. There was a significant correlation between protocol type and the number of GVs (p=0.04). Nine females with conventional protocol had 1 MI type oocyte and one of them had 4 MI oocytes. The number of MI oocytes was 7 in the double stimulation group, in which 5 females had 1 and 1 had 2 MI oocytes. After the second stimulation, three females had one MI oocyte and one had 5 MI oocytes in the double stimulation group.
Among the females with conventional protocol, four presented with 1 MII oocyte, 4 with 2 MII oocytes, 4 with 3 MII oocytes, and one with 5 oocytes in the ovaries. Among the females with double stimulation protocol, 5 had 1 MII oocyte, 10 had 2 MII oocytes, one had 3 MII oocytes, 4 had 4 MII oocytes and one of the females had 6 MII oocytes in the ovaries. After the second stimulation, six females presented with MII oocytes, one with 2 and one with 3 MII oocytes in the double stimulation group.
The mean number of oocytes retrieved was 2.76±1.9 in the conventional method and 3.23±2.1 in the double stimulation group (p=0.90). The number of fertilized oocytes was 31 in the conventional protocol and 25 in the double stimulation protocol. The mean number of pregnancies that led to the fetus was 1.38 ±1.3 in the conventional protocol and 0.96±0.9 in the double stimulation group (p=0.018); however, 4 pregnancies in the double stimulation group led to giving birth and only one in the conventional group gave birth to a child (p=0.016) (Table 2).
Discussion
In this clinical trial, it was aimed to compare the conventional method of antagonist with a high dose of gonadotropins with a double stimulation protocol. The evaluated patients all were considered as having POR and underwent ART.
For a positive outcome, the number and quality of oocytes are essential factors. In this study, the overall number of oocytes in the double stimulation protocol was higher than in the conventional method. However, neither the number of follicles nor the number of mature follicles differed significantly between the two studied groups.
On the other hand, studies have shown that the quality of the embryo is more important, thus some of the cells may not reach the blastocyst stage or fetus stage (13) mature oocytes collected, fertilization rate, blastocyst rate, biopsied blastocyst rate and euploidy rate. RESULTS: The double stimulation protocol had a significant higher number of oocytes collected (p=0.007). In this study, the mean number of blastocysts did not significantly differ between the two groups of study; however, the rate of positive outcome and giving birth was significant in females who underwent double stimulation protocol.
Ubaldi et al and Kuang et al (10,14) ongoing pregnancy rate, and implantation rate after frozen embryo transfer (FET both evaluated the efficacy of the double stimulation protocol by comparing the two stages of ovarian stimulation and found a significant improvement in the number and outcome of oocytes by this protocol.
In a similar study by Cardoso et al, the females who underwent double stimulation protocol were compared with those who received conventional ovarian stimulation (13) mature oocytes collected, fertilization rate, blastocyst rate, biopsied blastocyst rate and euploidy rate. RESULTS: The double stimulation protocol had a significant higher number of oocytes collected (p=0.007, and they had a significantly higher number of oocytes collected and mature oocytes. However, no statistically significant difference was found in fertilization and blastocyst rates.
Mild ovarian protocols were developed to extend the FSH gate through the administration of exogenous FSH during the mid-to-late follicular phase (14). The strategy of administering low doses of FSH in this period resulted in fewer oocytes with compatible pregnancy rates. A few trials have compared the long agonist stimulation with the mild stimulation in patients with normal ovarian reserve. Hohmann et al compared three protocols: a long agonist protocol (group A, n=45), a mild protocol that began rFSH on cycle day 2 (group B, n=48), and another mild protocol that began rFSH on cycle day 5 (group C, n=49). In group C, shorter stimulation and a lower total dose of gonadotropin were reported with no difference in the pregnancy rates (15). In another study, mild stimulation started with 150 IU/day rFSH beginning on day 5 of the cycle and the other group received long agonist stimulation starting with 225 IU/day rFSH (16). The ongoing pregnancy rate per cycle was not significant among the groups (17). In this study, the groups were significantly different in terms of stimulation period (days) and total gonadotropin dose (rFSH). However, the pregnancy and fertilization rates were similar between the groups, which aligns with the literature. Fresh single embryo transfer was used and there were no significant differences among the groups in terms of several retrieved oocytes, as well as the number and quality of oocytes/embryos. Casino et al reported similar pregnancy rates with the mild stimulation protocol in both fresh and thaw IVF cycles (18).
The double stimulation protocol has been introduced to improve the number of collected oocytes in a short period. It has been hypothesized that the luteal phase may affect the oocyte’s ability to mature and be fertilized without changing its capability of being fertilized (19,20). However, in this study, the number of oocytes did not significantly differ from the conventional method and the number of fertilized oocytes was greater in the conventional protocol.
Although we have observed insignificant differences in the number of oocytes and blastocysts, the embryos in the double-stimulation group were more capable of completing the pregnancy to give birth. While no significant difference was found in the endometrial thickness, this could be due to the quality of embryos or maternal factors in the double stimulation group.
In poor responders, RCTs comparing the short GnRH agonist vs. the GnRH antagonist regimen yielded contradictory and variable results (21). The inconsistency in results could be attributed to differences in the definition of poor response across studies. Griesinger et al conducted a meta-analysis on the use of GnRH agonist vs. antagonist in poor responders and discovered that the GnRH antagonist flexible dose regimen produced more oocytes than the long agonist regimen (22,23). Another meta-analysis comparing GnRH agonist vs. GnRH antagonist use in poor responders found no significant difference in efficacy between the two regimens (24).
Among the females who received high doses of gonadotropin, only one could give birth to a child. Land et al studied the results of a high dose of gonadotropin stimulation in 126 females with POR (25)126 poor response patients had a first treatment cycle on three ampules and a second cycle on six ampules of hMG per day. MAIN OUTCOME MEASURES: Numbers of follicles, oocytes, and embryos, and pregnancy rates. RESULTS: On six ampules, patients had significantly more follicles and oocytes. The number of embryos did not differ significantly. The pregnancy rate on six ampules were low (3.2% pregnancies per cycle started. Similar to the current study’s findings, they concluded that the rate of reproduction in females with POR is poor and that they do not benefit from high-dose HMG stimulation.
Limitations
In this study, for double stimulation protocol, the patients should have done two surgeries, but it was difficult for the patients to accept this.
Conclusion
The results of this study showed that the embryos in the double-stimulation group were more capable of completing the pregnancy, and the double-stimulation group had a more live birth rate.
Acknowledgement
The authors would like to thank all the individuals who allowed us to use their medical records. We also would like to acknowledge our colleagues at the Avicenna Research Institute. This study has a revised grant from the Avicenna Research Institute. Registration ID in IRCT:IRCT20180219038792N1, approval date:2019-01-02, and ethical code was IR.ACECR.Avicenna.REC.139t.1V.
Conflict of Interest
There was no conflict of interest in this manuscript.