Document Type : Original article
Abstract
Background: In this study, Cone-Beam Computed Tomography (CBCT) was used to assess the dimension and posture of the tongue, as well as Alveolar Bone Thickness (ABT) and labiolingual inclination of mandibular central incisors in order to look for any correlations.
Methods: A total of 200 CBCT images of skeletal Class I and II individuals were studied. Each group of malocclusion was divided into three subgroups: low-angle, normal-angle, and high-angle. Buccal and lingual alveolar bone thickness (BT & LT), and the Inclination of Mandibular Plane Angle (IMPA) were measured and compared by using T-test. The spearman rank correlations test analyzed the correlations between dental variables and tongue measurements (p<0.05).
Results: Significant weak correlations were identified between dental variables and tongue measurements. In Cl I malocclusion, IMPA and Tongue Length (TGL) were found to be significantly correlated with a correlation value of 0.324 (p=0.001). In Cl II malocclusion, there was a significant correlation between BT3 and TGH. About BT3, there was a significant correlation with D4’ and a negative correlation with D5’. Further comparison among vertical subgroups revealed the same results.
Conclusion: Class I patients with superior tongue posture may have thicker lingual alveolar bone around mandibular incisors and Class II patients showed that thicker labial alveolar bone of lower incisor and thinner alveolar bone at the lingual side may be associated with a superior position of the posterior portion of the tongue.
Keywords: Alveolar bone, Angle Class I, Angle Class II, Cone-Beam Computed Tomography, Malocclusion
Introduction
Dental and skeletal malocclusions may develop due to genetic and environmental factors (1). Based on the functional matrix theory, growth of the craniofacial skeleton is controlled by the surrounding soft tissue (2). Tongue is one of the most critical elements of the orofacial soft tissue functional matrix, and its resting position has a causative role in development of malocclusion. It is also an important factor to consider in orthodontic treatment planning and stability of the results (3). The tongue position has been previously assessed in different individuals by means of measurements on lateral cephalograms. Fatima and Fida found no significant difference in tongue posture among individuals with different sagittal skeletal patterns of the jaw (4). However, Chauhan et al reported that individuals with Class II division 1 malocclusion had higher tongue postures than Class I individuals, and Primozic et al found a significantly lower tongue posture in Class III compared with Class I individuals (5,6). Considering the inconsistency in the results of studies that used two-dimensional radiographic modalities, more recent investigations used three-dimensional (3D) Cone-Beam Computed Tomography (CBCT) to obtain more accurate results. Recent studies reported a lower tongue posture in skeletal Class II individuals (1,7). Also, forward tongue posture and increased tongue length were shown to be associated with flared incisors (8,9).
Inclination of the anterior teeth is also influenced by different malocclusion patterns and affects the Alveolar Bone Thickness (ABT) (10). ABT dictates the limits of orthodontic tooth movement, and should be considered in order to prevent periodontal tissue damage and occurrence of dehiscence, fenestration, and gingival recession (11). Studies on 3D images demonstrated that the thickness of buccal alveolar bone at the site of lower incisor was greater in Class I than Class II and Class III individuals (12-14). Furthermore, the comparison among Class II individuals with different vertical growth patterns has revealed that patients with a high-angle pattern had thinner labial alveolar bone covering mandibular central incisors than those with normal-angle or low-angle patterns (15).
As mentioned earlier, the dimensions and position of the tongue in different skeletal malocclusions have been the topic of many investigations. Also, the ABT surrounding the anterior teeth in different sagittal growth patterns has been previously studied. However, to the best of the authors’ knowledge, the relationship between the tongue variables and inclination of mandibular anterior teeth or the ABT in this region has not been investigated to this date. Therefore, the purpose of this retrospective study was to use CBCT data to evaluate the correlation between the lower central incisor inclination and ABT in this region with tongue dimensions and posture in Class I and Class II skeletal malocclusion.
Materials and Methods
The association between the posture of the tongue and the ABT and lower central incisor inclination in Class I and Class II skeletal patterns was assessed in this retrospective cross-sectional investigation using the CBCT images. 609 adult patients’ CBCT scans from 2016 to 2021 were selected at random from the archives of two oral and maxillofacial radiology facilities. All the CBCT scans had been obtained for reasons unrelated to the current investigation. No participant was therefore exposed to any additional radiation dosage, and the patients’ personal information was not recorded. The sample size was calculated to be at least 87 cases for each group assuming alpha=0.05, beta=0.2 (80% power), and r=0.05 using the power analysis of IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA).
This study was approved by the Ethics Committee of Shahid Beheshti School of Dentistry (ethical ID: IR.SBMU.DRC.REC.1400.39).
The following inclusion criteria were used to choose 200 CBCT scans in total
(I) Patients over the age of 18, (II) complete permanent dentition up to the second premolars and the absence of at most one first or second molar in each arch, (III) CBCT images obtained with the tongue at rest and a distance from the palate, (IV) CBCT images with a 15×15 cm field of view, and (IV) patients with no or minor crowding (maximum crowding of 4 mm in each arch).
The exclusion criteria were
(I) A history of orthodontic or orthopedic procedures, (II) dental or craniofacial malformations, (III) a history of a syndrome or trauma, (IV) congenitally absent or supernumerary teeth, (V) considerable tooth rotation, and (VI) significant skeletal asymmetry.
The CBCT images were obtained with the tongue at rest and at a distance from the palate in maximum intercuspation by using the NewTom VGI CBCT scanner (Verona, Italy). The exposure parameters were 100 kVp and 150 mA for all the CBCT scans. To import the DICOM files of the CBCT scans and reconstruct the image sections for evaluation, OnDemand 3D software was used (version 1.0.10.6388).
The patients were divided into 2 equal groups, each consisting of 100 patients (a total of 200 patients), according to their sagittal skeletal pattern:
1) ANB (02) Wits (-1Additionally, in each sagittal group, the significant associations were once more examined across the three vertical subgroups (based on Jarabak’s ratio: 62 to 65%, normal; >65%, low angle; <62%, high angle).
Next, the right side of the face was cropped on the coronal view, and the structural planes were analyzed on the 3D view (synthesized lateral cephalograms) to avoid overlapping.
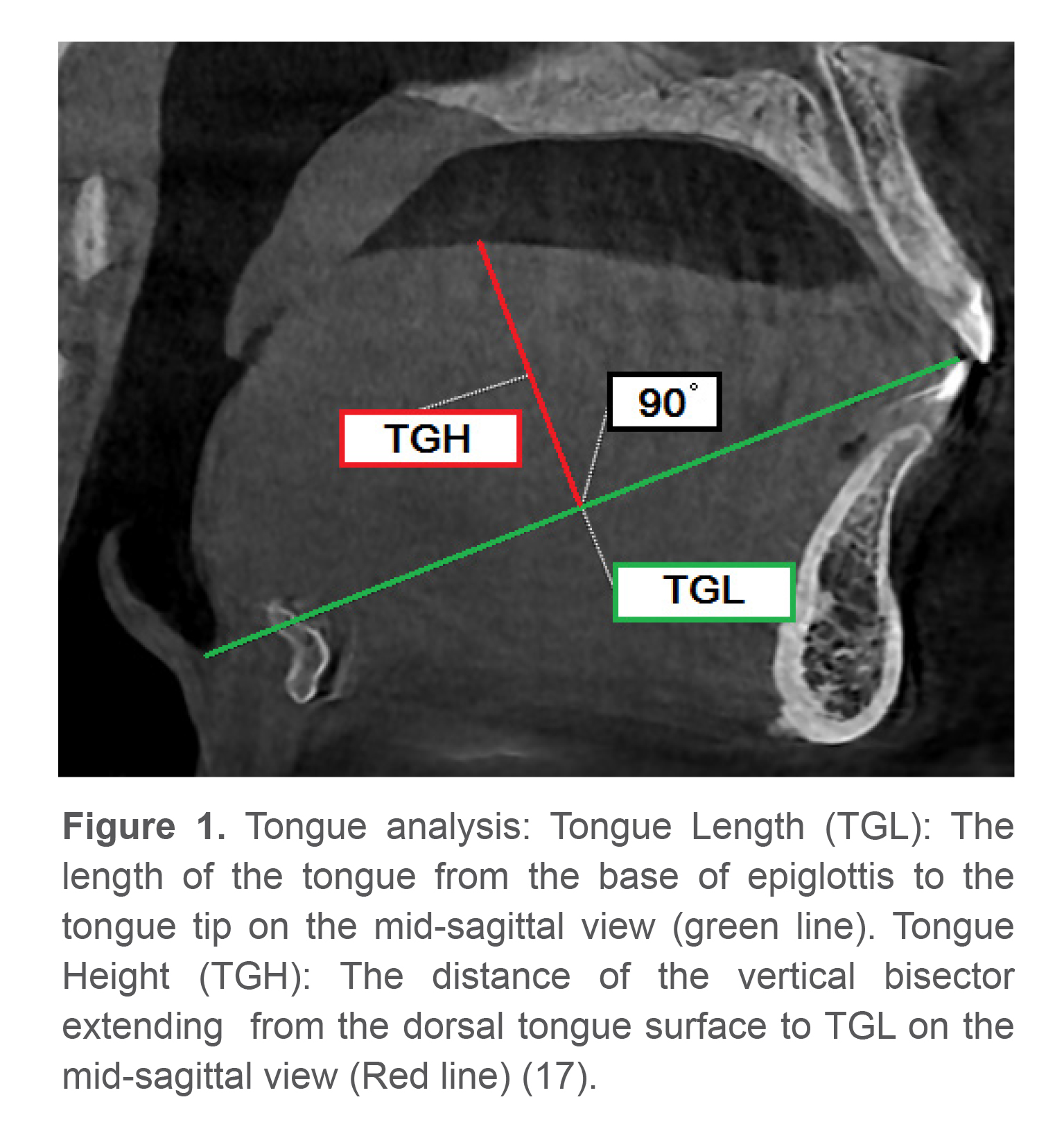
Tongue analysis
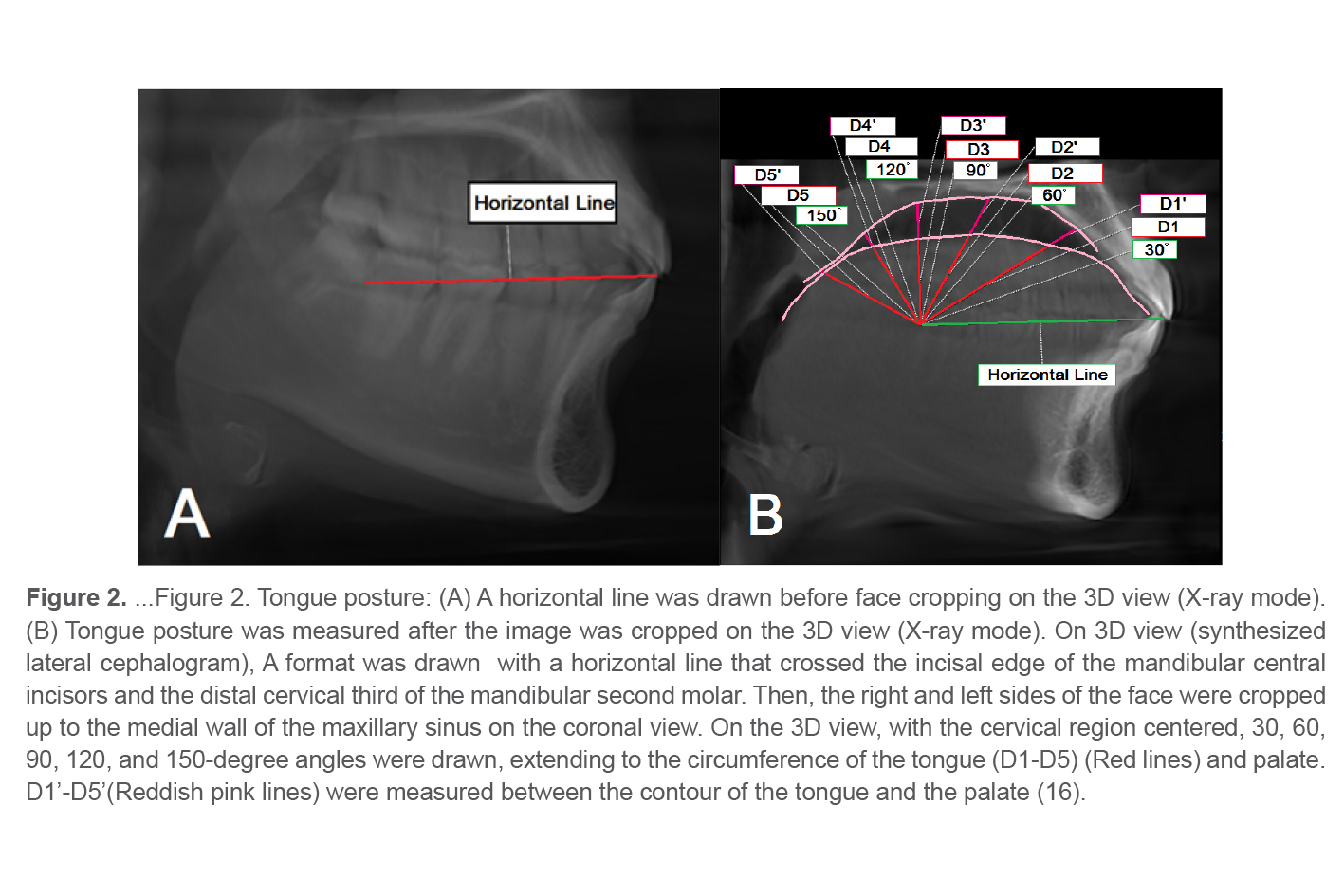
The measurements used to assess the tongue dimensions included the tongue length and height (mm) (Figure 1). The position of the tongue was assessed using a model based on the Graber analysis (16) (Figure 2).
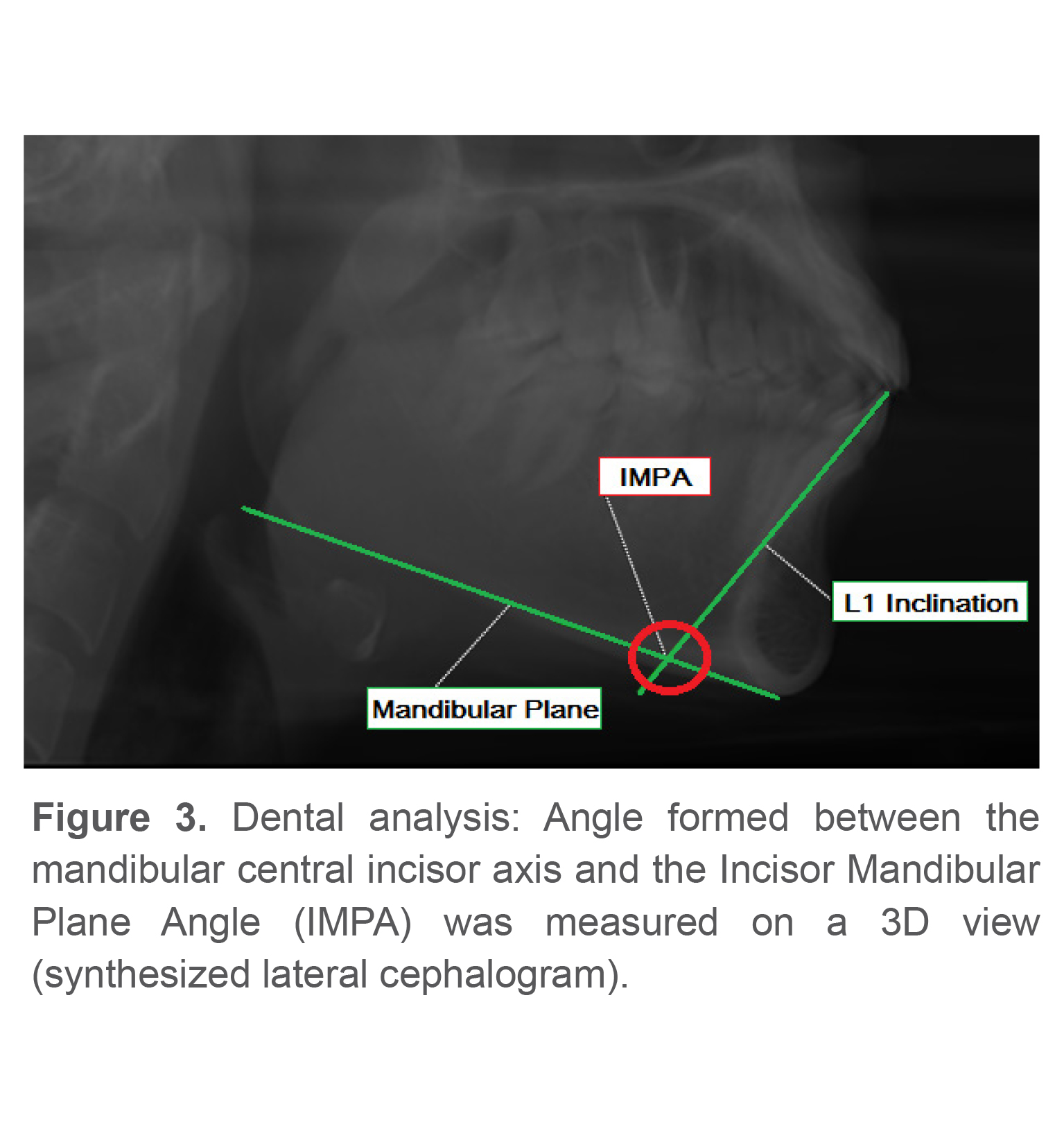
Dental analysis
Landmark identification and measurement of the inclination of mandibular central incisors were performed according to the Steiner analysis (Figure 3) (18,19).
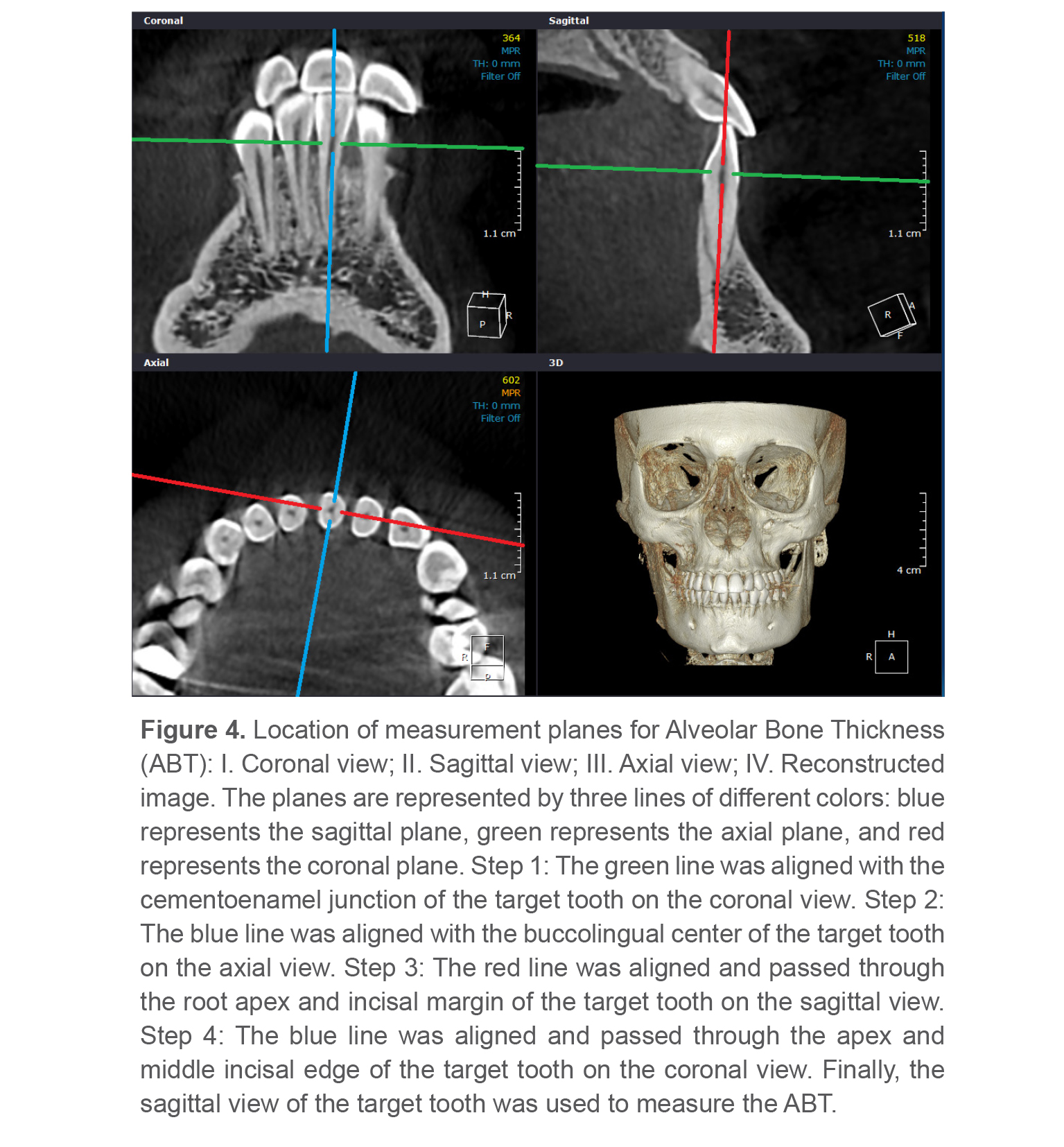
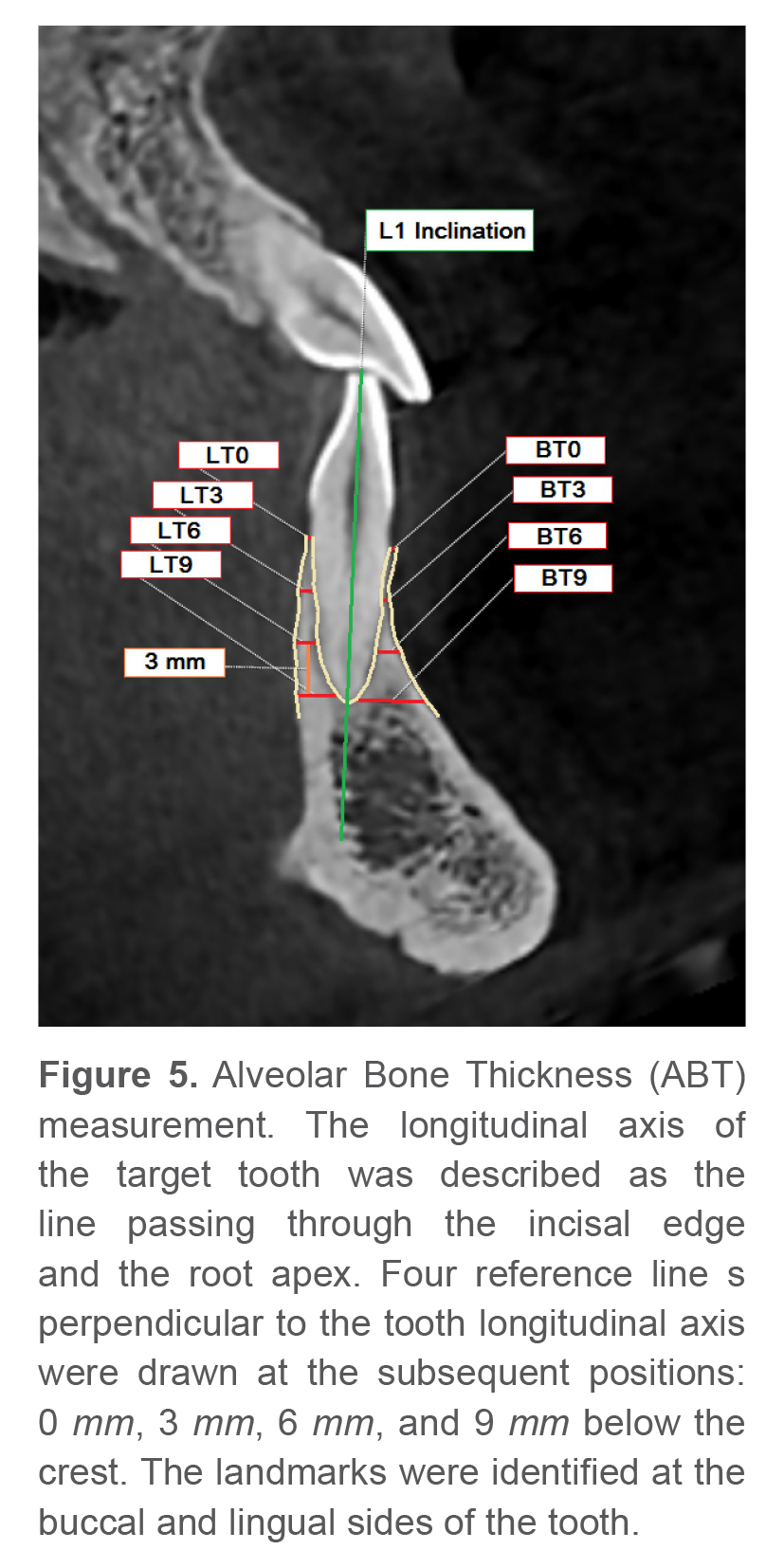
Figure 4 shows the procedure used to find the ABT measurement plane. The sagittal plane was defined as the reference plane, centered at the buccolingual midpoint of the target tooth. The right and left mandibular central incisors were selected as the target teeth and the mean value of the two measurements was used for further analysis (Figure 5).
Under identical circumstances and using the same system, two examiners were calibrated for the measurements. 20 patients were randomly chosen from the entire sample, and the measurements were repeated for them by the same examiner after a 2-week interval in order to evaluate the measurement’s reliability. The intra-examiner reliability was evaluated using the T-test and the Intraclass Correlation Coefficient (ICC). Between the two examiners, the inter-examiner reliability was also calculated (Table 1).
Statistical analysis
First, the mean ABT values were determined for the locations of the right and left mandibular central incisors. The normality of data distribution was examined using the Kolmogorov-Smirnov test. For each side (buccal and lingual) and level (0, 3, 6, and 9 mm apical to the crest), the values of the mean and standard deviation were presented. ABT was compared between the two sagittal groups of the patients by using t-test. The correlations between the tongue posture and tooth variables were analyzed by the Spearman’s correlation test (p<0.05).
Results
The majority of the data had a normal distribution as shown by the Kolmogorov-Smirnov test.
Table 2 indicates that there are no statistically significant differences by gender and mean age of the patients with different sagittal and vertical groups (p>0.05).
The ABT at the site of the lower central incisors was compared between Class I and Class II malocclusion patients. The descriptive statistics and intergroup comparisons are shown in table 3. No statistically significant differences were found between the two groups. But, IMPA in Class II patients was significantly greater than that in Class I patients (p=0.000).
Some statistically significant correlations were observed between the tongue variables (posture, height and length) and tooth variables (IMPA and ABT) of mandibular central incisors in 2 sagittal and Class I and Class II groups (p<0.05, Table 4).
IMPA had a statistically significant correlation with tongue length in Class 1 skeletal pattern (r = 0.324; p=0.001), but there was no significant correlation in Class II skeletal pattern.
ABT at the crest
In Class I individuals, a significant inverse correlation was observed between the tongue height and ABT in labial and lingual sides (p<0.05).
ABT at 3 mm apical to the crest
In Class I individuals, a statistically significant correlation was observed between D5 and ABT in the lingual side. Also, a statistically significant inverse correlation was observed between D3’ and ABT in the lingual side.
In Class II individuals, a statistically significant correlation was observed between (TGH, D4’) and ABT in the labial side. Also, a statistically significant inverse correlation was observed between D5’ and ABT in the labial side.
ABT at 6 mm apical to the crest
In Class II individuals, a statistically significant correlation was observed between D5’ and ABT in the lingual side.
ABT at 9 mm apical to the crest
There was no statistically significant correlation between the tongue posture and ABT on either side.
In addition, significant correlations were analyzed again in 6 groups according to their sagittal and vertical skeletal patterns (p<0.05, Table 5).
Table 1. Intra- and inter-examiner reliability values
|
|
Intraclass correlation coefficient |
95% confidence interval |
Mean difference |
Std. Deviation |
p-value |
|
Intra-examiner |
0.91 |
0.79-0.92 |
-0.03 |
1.242 |
0.871 |
|
Inter-examiner |
0.94 |
0.80-0.94 |
0.09 |
0.683 |
0.592 |
Table 2. Age and gender of the patients in sagittal and vertical groups
|
Variable
|
Class I |
Class II |
Total |
p-value |
|||||
|
Low angle |
Normal |
High angle |
Low angle |
Normal |
High angle |
||||
|
Gender, n |
Female |
23 |
20 |
17 |
21 |
15 |
20 |
116(58%) |
0.701a |
|
Male |
14 |
13 |
13 |
15 |
18 |
11 |
84(42%) |
||
|
Total (%) |
37(18.5) |
33(16.5) |
30(15) |
36(18) |
33(16.5) |
31(15.5) |
200(100%) |
||
|
Age (y) |
31.98±8.99 |
35.01±11.63 |
32.96±1.77 |
0.881b |
|||||
a Results of Chi-square test; b Results of Student t-test
Age is presented as mean±standard deviation.
Table 3. Comparison of ABT at the site of mandibular central incisors between skeletal Class I and skeletal Class II malocclusion patients (mm)
|
Side |
Position† |
Sagittal Group |
p-value |
|
|
Class I |
Class II |
|||
|
Buccal |
0 |
0.21±0.13 |
0.23±0.22 |
0.875 |
|
3 |
0.32±0.22 |
0.36±0.31 |
0.396 |
|
|
6 |
0.79±0.60 |
0.86±0.69 |
0.752 |
|
|
9 |
2.63±1.34 |
2.65±1.71 |
0.569 |
|
|
Lingual |
0 |
0.19±0.11 |
0.19±0.12 |
0.742 |
|
3 |
0.52±0.41 |
0.50±0.39 |
0.654 |
|
|
6 |
1.17±0.72 |
1.03±0.61 |
0.320 |
|
|
9 |
2.62±1.11 |
2.36±0.92 |
0.175 |
|
Values are presented as mean±standard deviation.
† Apical distance from crest in mm; *p-value<0.05
Table 4. The statistically significant correlations between the tongue variables and alveolar bone thickness and IMPA in Class I and Class II skeletal patterns
|
Class I |
Class II |
||||
|
Tongue ABT /IMPA |
Correlation coefficient |
p-value |
Correlation coefficient |
p-value |
|
|
TGH |
TGH |
||||
|
BT0 |
-0.218 |
0.029 |
BT3 |
0.241 |
0.016 |
|
BT3 |
-0.207 |
0.038 |
|||
|
LT0 |
-0.235 |
0.018 |
D4’ |
||
|
TGL |
BT3’ |
0.202 |
0.044 |
||
|
IMPA |
0.324 |
0.001 |
|||
|
D5 |
D5’ |
||||
|
LT3 |
0.210 |
0.036 |
|||
|
D3’ |
BT3 |
-0.198 |
0.048 |
||
|
LT3 |
-0.223 |
0.026 |
LT6 |
0.206 |
0.040 |
*Spearman’s correlation test
Table 5. Statistically significant correlations between the tongue variables and alveolar bone thickness and IMPA among Cl I and Cl II vertical subgroups
|
Cl I Low Angle |
Cl II Low Angle |
||||
|
Tongue ABT /IMPA |
Correlation coefficient |
p-value |
Correlation coefficient |
p-value |
|
|
TGL |
TGH |
||||
|
IMPA |
0.412 |
0.011 |
BT3 |
0.375 |
0.024 |
|
Cl I Normal |
D4’ |
||||
|
TGL |
BT3 |
-0.375 |
0.032 |
||
|
IMPA |
0.453 |
0.008 |
|||
|
Cl I High Angle |
D5’ |
||||
|
TGH |
LT6 |
0.352 |
0.035 |
||
|
BT0 |
-0.418 |
0.022 |
|||
*Spearman’s correlation test
Discussion
Inclination of lower incisors is important in orthodontics, since it can affect treatment planning and serve as a predictor of the stability of the orthodontic treatment results (20). Due to the thickness of the alveolar bone, lower incisors have a limited range of movement anteroposteriorly; hence, the tipping movement comprises the majority of the lower incisor movements that take place during the orthodontic treatment (21). Attention must be paid to the position of lower incisors as well as the ABT at the site to avoid adverse consequences such as root resorption, gingival recession, and/or fenestration.
The correlation of the shape and function of the stomatognathic system has been the topic of many investigations. It has been hypothesized that the location of teeth and other oral structures can be influenced by the tongue (22). According to the Tomes Theory, the position of the teeth is primarily determined by the perioral musculature and the tongue (23). However, to the authors’ knowledge, the relationship between the size and position of the tongue with lower incisor inclination and ABT has not yet been assessed.
Only a few techniques are available to assess the position and size of the tongue on radiographs. The measurements made on lateral cephalograms have been routinely employed for this purpose. This approach does not, however, provide a 3D image of the tongue and does not allow cross-sectional measurements (24). It has been claimed that magnetic resonance imaging techniques, which are more suitable for soft tissue evaluation, could be useful for tongue assessment, but there are a number of limitations to this approach, including its high cost, limited availability, lack of adequate cortical bone contrast, and the fact that it is not frequently utilized for orthodontic patients (9,24). In 1982, Roehm discussed that evaluation of the tongue with computed tomography (CT) was a reliable and effective approach (25). CBCT offers optimal 3D image quality comparable to that of medical CT, but with lower radiation exposure (26). Another advantage of CBCT is that the patient is seated upright during the procedure, preventing the tongue from collapsing (24). Numerous studies have demonstrated that CBCT not only offers precise data for tongue evaluation, but it may also provide an accurate and reliable method for measuring dental alveolar thickness (27). In the current study, CBCT was used for the tongue and ABT measurements.
In the present study, a statistically significant correlation was observed between the tongue length and lower incisor inclination in Class I group. This finding is in line with the results of Seden et al (8) who indicated increased tongue length in subjects with flared lower incisors. Lowe et al (28) also reported that short tongue length correlated with upright central incisors. The above-mentioned studies were conducted on Class I individuals.
No significant relationship was found between the tongue length and lower incisor inclination in individuals with skeletal Class II malocclusion. The present findings also indicated that Class II individuals had greater inclination of mandibular central incisors compared with Class I individuals, which is due to natural compensation for the underlying skeletal discrepancy. The authors believe that independence of lower incisor inclination from the tongue length in this group is due to this compensation, which causes the mandibular incisors to flare irrespective of the tongue length. However, the ABT of mandibular central incisors remain constant despite increased inclination as demonstrated by our findings which show no significant difference among Class I and Class II subjects considering mandibular incisor ABT.
Chakraborty et al (11) found that Class II individuals had lower resting tongue pressure compared with Class I patients. The independence of lower incisor inclination from the tongue length in Class II individuals may also be explained by the reduced tongue pressure.
The present findings showed no correlation between the tongue posture or height and lower incisor inclination. According to Proffit, the opposing forces of the tongue and lips are not the only factors affecting the equilibrium defining the tooth position; this statement provides an explanation for the abovementioned observations (29). Factors affecting the mandibular incisor inclination include, but are not limited to, head posture, hyoid position, symphyseal patterns, compensations related to skeletal malocclusion, and forces generated within the periodontal membrane (8,29,30). According to a study by Seden et al, a more flexed head posture and a hyoid bone that is situated closer to the symphysis are both associated with proclined mandibular incisors (8). Also, Gutterman et al pointed to the association of lower incisor inclination with symphyseal depth, and the patient’s sex, age, and skeletal vertical pattern (30).
ABT is an important limiting factor in orthodontic tooth movement, and fenestration and/or dehiscence may occur if adequate attention is not paid to ABT (31).
The correlation between ABT at the site of mandibular central incisors and tongue posture and dimensions was also evaluated in the present study. At 3 mm apical to the crest in the lingual side of the lower central incisor, ABT had a significant correlation with D5, which corresponds to the tongue height in the posterior region, and inverse correlation with D3’, which corresponds to the distance from the tongue to the palate in the middle tongue portion, in Class I individuals. Such results suggest that patients with a superior tongue posture may have thicker lingual alveolar bone covering their mandibular central incisors.
In Class II patients, D5’ had a correlation with the lingual ABT at 6 mm apical to the crest and a weak inverse correlation with buccal ABT at 3 mm apical to the crest of the mandibular central incisor. Such findings imply that thicker alveolar bone at the labial side of the lower incisor and thinner alveolar bone at the lingual side might be associated with a superior position of the posterior portion of the tongue. However, the relationship between the tongue posture and ABT should be interpreted with great caution, as the discovered correlations were weak.
Considering the weak correlations found between the tongue variables and the mandibular incisor inclination and ABT, the authors assume that a compensating mechanism within the dentoalveolar system counteracts the effects of the tongue and maintains the inclination and the covering bone thickness of the lower central incisors within a constrained range. Another presumption is that other variables that affect ABT, as past research has indicated, likely outweigh the effects of the tongue. The vertical growth pattern and the transverse jaw relationship have been identified as variables impacting the lower incisor ABT in the investigations by Dalaie et al and Qu et al, respectively (15,27)
Conclusion
1. Class I patients with a superior tongue posture may have thicker lingual alveolar bone covering their mandibular central incisors.
2. Class II patients showed that thicker alveolar bone at the labial side of the lower incisor and thinner alveolar bone at the lingual side may be associated with a superior position of the posterior portion of the tongue.
3. Significant weak correlations were found between the tongue variables and the mandibular incisor inclination and ABT. This finding presupposes a compensating mechanism within the dentoalveolar system counteracts the effects of the tongue and maintains the inclination and the covering bone thickness of the lower central incisors within a constrained range.
Acknowledgement
This study was approved by the Ethics Committee of Shahid Beheshti School of Dentistry (ethical ID: IR.SBMU.DRC.REC.1400.39).
Conflict of Interest
There was no conflict of interest in this manuscript.