Document Type : Original article
Introduction
According to statistics presented by United Nations under the title of world population prospect, Iran is the 18th most populous country all over the world by estimated population of 81 million in July 2017 1. The mid age has been reported 30 in urban areas, 28 in rural areas and 30 in total population. According to the reports of national Statistical Center of Iran, the first age group of 4, that includes population aged up to 14, exceeded 45% of total population in 1986, while it has decreased to 24 percent in 2016 2. However, although the ratio of this group has reduced for more than 21%, its total population did not diminish for more than 3 million, because of raw population growth. Bushehr is the 23rd populous province of Iran; however it has the second level of population growth and predicted to face a great increase in the population of children and adolescence during coming years 2.
Different studies around the world have estimated the prevalence of psychiatrics’ disorders among children and adolescents. The calculated figures vary from 3.5 up to 34% in different countries that have been discussed separately 3,4. Although the huge population of children and adolescents in Iran, only few studies have been conducted on prevalence of psychiatrics’ disorders among them. There are different related reports since 2009 from Iran, including the study of Moharreri et al 5 that presented the prevalence of 34 percent in cases aged 6 to 18 in the city of Mashhad, and the study of Mohammadi et al 6 that explained the prevalence of 10.55 percent among the similar samples in five large cities of Iran including Tehran, Mashhad, Tabriz, Isfahan and Shiraz. The data about prevalence of psychiatric disorders in Bushehr province is lacking.
The investigators of this study designed a local survey to investigate the prevalence of mental and psychiatric disorders among Bushehr ’s children and adolescents, and their comorbidities.
Materials and Methods
This population-based study was designed in a cross sectional form based on the stratified random cluster sampling to draw the profile of psychiatric disorders among children and adolescents in Bushehr. According to census of 2016, Bushehr Province’s population was 1,161,400 that up to 68.2% were residents of urban areas. The population density of this province had been 51/km 2, and Bushehr has the second rate of population growth among all of the provinces in Iran 2. The study was conducted in the capital city of this province and its suburb rural areas. To achieve a uniform random distribution in the areas under study, the sampling was administered through postal code with the help of post office in both urban and rural areas. The cases were chosen among Iranian citizens who were between 6 to 18 years old and resided for at least one year at Bushehr Province (inclusion criterion). The children and adolescents affected by severe physical disorders were excluded (exclusion criterion).
Two main questionnaires were used in this survey; (1) a self-report semi-structured questionnaire to gather familial and demographic information included age, gender, residential area, parental job and parental education levels. (2) Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS-PL) to detect psychiatric disorders in children and adolescents. The K-SADS is a screening tool for detection of childhood and adolescence mental disorders. This semi-structured instrument which is created to assess children aged 6 to 18, has 4 versions. The Present and Lifetime Version (KSADS-PL) of this inventory has been firstly presented by Kaufman, Birmaher, Brent, Rao and Ryan in 1996 and is used in our study 7. This comprehensive instrument is efficient in screening a great variety of psychopathologies including Major Depressive Disorder, Mania, Bipolar Disorders, Schizophrenia, Schizoaffective disorder, Obsessive Compulsive Disorder, Generalized Anxiety Disorder, Eating Disorders, Attention Deficit Hyperactivity Disorder, Conduct Disorder, Post Traumatic Stress Disorder, etc. This version consists of six parts: Unstructured Introductory Interview – Developmental History that asks about basic information such as birth and developmental history, previous and current physical and mental problems, and relations with friends, family members and schoolmates. The second part is Diagnostic Screening Interview that assesses serious symptoms since past so far, by scoring protocol and probes. The next part is Completion Checklist Supplement for screening of rest of the disorders. Appropriate Diagnostic Supplements seeks for the existence of symptoms for non-psychotic non-affective disorders. The fifth section which is Summary Lifetime Diagnosis Checklist summarizes the data extracted by previous parts. The last part is Children’s Global Assessment Scale for investigation of child’s functionality. The reliability and validity of this semi-structured questionnaire has been first confirmed by Kaufman et al 7 who reported a test-retest reliability of 0.77-1.00 and the inter-rater agreement of 93-100% for lifetime and present diagnosis of psychiatric disorders. However, the Persian Version of K-SADS-PL was used in our assessments. The acceptable characteristics of Persian Version of KSADS-PL among Iranian children have been proven by Ghanizadeh et al in 2008 8. The reported test-retest and inter-rater reliabilities for the Persian version of K-SADS-PL were 0.56-0.81 and 0.69, respectively 8. Moreover, other reliable instruments were used to distinguish mental retardation, epilepsy, and tobacco use.
Eight clinical psychologists trained by a psychiatrist to complete the K-SADS-PL were referred to the houses. After describing the study protocol and consenting to participate, children and their parents were involved into the study. Interviews were conducted by two interviewers with children and their parents simultaneously, especially with their mothers, and a summary rating was entered according to the agreement of two interviewers. The readers can refer to the study protocol, which is previously published, to find more details about the method of implementation of this survey 9. After gathering information, data were entered into the SPSS software (version 20, IBM Corporation, United States) and analyzed using descriptive and analytical statistics. The study was funded by the National Institute for Medical Research Development (NIMAD, grant No. 940906).
Ethical considerations
All the parents and adolescences aged 15 and above studied and signed consent forms describing the purpose of our project and its potential beneficial effects on public mental health. They were informed that their personal information will remain confidential, and they can quit the assessments if they found it undesirable. The team was committed to treat the cases that obtained psychiatric diagnoses following the evaluations, free of charge, or refer them to other experts, based on their will. The ethics review board in the NIMAD has approved the study protocol (the ethics code: IR.NIMAD.REC.1395.001).
Results
The sample size of our study was 1037. They were aged between 6 up to 18, including 502 male (48.4%) and 537 (51.6) female samples. They were categorized into 3 age groups; the group of children aged between 6 to 9 years old that had 353 members, the group of adolescents’ aged 10 to 14 covered 349 cases, and the group of teenagers 15 to 18 years old gathered 335 samples, equal to 34, 33.7 and 32.3% of all, respectively. Up to 93.6% of cases (n=971) were residents of urban areas.
According to assessments, 11.6% of total cases including 10.2% of boys and 12.9% of girls, which means 51 male and 69 female cases were detected to have any kind of diagnoses. Among these 120 affected cases, 41, 32 and 47 patients belonged to the first, second and third age categories, equal to 11.6, 9.2 and 14% of each group, respectively. 12.3% of urban cases were affected by psychiatric disorders (n=119) versus one case (1.5%) of children and adolescents residing in rural areas.
The educational status of parents was recorded by a sequential grading scale, including: Illiterate, Primary school, Guidance & high school, Diploma, Bachelor, and master degree or above. The most frequent degree among both of the parents was high school diploma, by 34.3% of mothers and 29.4% of fathers. The least frequent educational levels were illiteracy among fathers (4.2%) and Master degree or above among mothers (3.6%). The most frequent educational level among fathers and mothers were ‘bachelor’ and ‘high school diploma’.
Considering the occupational issues, 46.4% (n=469) of fathers and 11.1% (n=113) of mothers were employed in public/governmental organizations, while 51.3% (n=518) and 3.3% (n=34) of them worked in private businesses. Only 2.3% of fathers (n=23) were unemployed, however up to 85.6% of mothers (n=827) worked as housewives. The highest frequencies of psychiatric disorders in children were among who had unemployed fathers or mothers working in governmental organization, versus lowest prevalence among the children of fathers occupied in public sectors or mothers working in private businesses (Table 1).
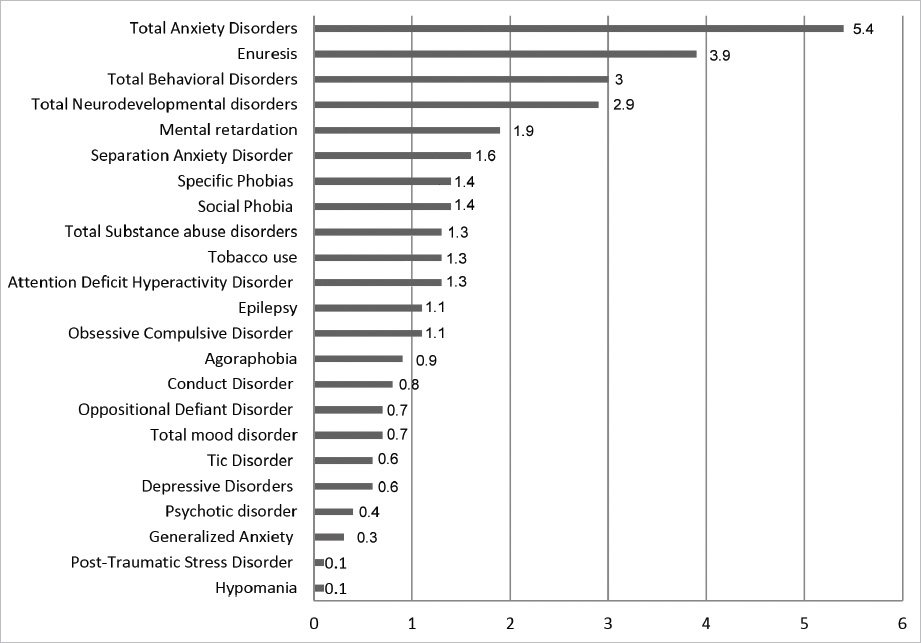
Among 120 cases with psychiatric diagnoses, anxiety disorders as a whole were the most frequent psychopathology, affecting up to 5.4% of total population. The subgroups of this category were separation anxiety, social and specific phobias, obsessive compulsive disorders, agoraphobia, generalized anxiety and post-traumatic stress disorder, sorted from highest to lowest prevalence.
After enuresis that was the second frequent complaint among children, behavioral disorders and neuro-developmental disorder reached 3rd (3%) and 4th (2.9%) places. The category of behavioral disorders contained attention deficit hyperactivity, conduct oppositional defiant and tic disorders respective to decrease of prevalence. The category of neuro-developmental disorder included mental retardation and epilepsy. The substance abuse, mood disorders and psychotic disorders were the least prevalent categories by affecting 1.3, 0.7 and 0.4% of cases, respectively (Table 2).
The prevalence of comorbidities has been also investigated. The most common comorbidity of anxiety disorder is enuresis (14.3%) while anxiety itself is the most frequent comorbidity of behavioral and neurodevelopmental disorders (Table 3, Figure 1).
Table 1. Frequency of demographic variables
|
Confidence Interval (95%) |
Affected cases |
Total cases |
|
|||
|
p |
n |
P |
N |
|||
|
7.81-13.11 |
10.2 |
51 |
48.4 |
502 |
Male |
Sex |
|
10.32-16.01 |
12.9 |
69 |
51.6 |
535 |
Female |
|
|
8.67-15.37 |
11.6 |
41 |
34 |
353 |
6-9 |
Age |
|
6.57-12.66 |
9.2 |
32 |
33.7 |
349 |
10-14 |
|
|
10.72-18.16 |
14 |
47 |
32.3 |
335 |
15-18 |
|
|
10.34-14.47 |
12.3 |
119 |
93.6 |
971 |
Urban |
Place of residence |
|
0.3-8.1 |
1.5 |
1 |
6.4 |
66 |
Rural |
|
|
6.72-27.85 |
14.3 |
6 |
4.2 |
42 |
Illiterate |
Father’s educational level |
|
8.67-21.23 |
13.8 |
16 |
11.5 |
116 |
Primary school |
|
|
10.18-20.07 |
14.4 |
28 |
19.3 |
194 |
Guidance & High school |
|
|
7.47-14.48 |
10.5 |
31 |
29.4 |
296 |
Diploma |
|
|
4.83-11.12 |
7.4 |
20 |
26.9 |
271 |
Bachelor |
|
|
7.98-22.34 |
13.6 |
12 |
8.7 |
88 |
MSc or higher |
|
|
|
- |
7 |
- |
30 |
Missing |
|
|
4.75-20.46 |
10.2 |
6 |
5.8 |
59 |
Illiterate |
Mother’s educational level |
|
11.64-23.3 |
16.7 |
26 |
15.3 |
156 |
Primary school |
|
|
8.76-17.85 |
12.6 |
26 |
20.2 |
206 |
Guidance & High school |
|
|
6.09-12.01 |
8.6 |
30 |
34.3 |
349 |
Diploma |
|
|
8.91-17.9 |
12.7 |
27 |
20.8 |
212 |
Bachelor |
|
|
4.41-25.31 |
11.1 |
4 |
3.5 |
36 |
MSc or higher |
|
|
|
- |
1 |
- |
19 |
Missing |
|
|
7.44-12.84 |
9.8 |
46 |
46.4 |
469 |
Public sector |
Father’s occupational status |
|
9.8-15.47 |
12.4 |
64 |
51.3 |
518 |
Private sector |
|
|
6.98-37.14 |
17.4 |
4 |
2.3 |
23 |
Unemployed |
|
|
|
- |
6 |
- |
27 |
Missing |
|
|
8.91-21.77 |
14.2 |
16 |
11.1 |
113 |
Public sector |
Mother’s occupational status |
|
1.63-19.09 |
5.9 |
2 |
3.3 |
34 |
Private sector |
|
|
9.62-13.87 |
11.6 |
101 |
85.6 |
872 |
Unemployed (Housewife) |
|
|
|
- |
1 |
- |
18 |
Missing |
|
|
9.8-13.7 |
11.6 |
120 |
100 |
1037 |
Total |
|
Table 2. Prevalence of psychiatric disorders
|
Psychiatric disorders |
Number |
Percentage |
Confidence Interval (95%) |
|
|
Mood disorders |
Depressive disorders |
6 |
0.6 |
0.3-1.26 |
|
Hypomania |
1 |
0.1 |
0.02-0.5 |
|
|
Total mood disorder |
7 |
0.7 |
0.3-1.39 |
|
|
Psychotic disorder |
4 |
0.4 |
0.15-1 |
|
|
Anxiety disorders |
Separation anxiety disorder |
17 |
1.6 |
1.03-2.61 |
|
Social phobia |
14 |
1.4 |
0.8-2.25 |
|
|
Specific phobias |
14 |
1.4 |
0.8-2.25 |
|
|
Agoraphobia |
9 |
0.9 |
0.5-1.64 |
|
|
Generalized anxiety |
3 |
0.3 |
0.1-0.9 |
|
|
Obsessive compulsive disorder |
11 |
1.1 |
0.6-1.89 |
|
|
Post-traumatic stress disorder |
1 |
0.1 |
0.02-0.6 |
|
|
Total anxiety disorders |
56 |
5.4 |
4.18-6.95 |
|
|
Behavioral disorders |
Attention deficit hyperactivity disorder |
13 |
1.3 |
0.7-2.13 |
|
Oppositional defiant disorder |
7 |
0.7 |
0.3-1.39 |
|
|
Conduct disorder |
8 |
0.8 |
0.4-1.51 |
|
|
Tic disorder |
6 |
0.6 |
0.3-1.26 |
|
|
Total behavioral disorders |
31 |
3 |
2.11-4.21 |
|
|
Neurodevelopmental disorders |
Mental retardation |
20 |
1.9 |
1.25-2.96 |
|
Epilepsy |
11 |
1.1 |
0.6-1.89 |
|
|
Total neurodevelopmental disorders |
30 |
2.9 |
2.03-4.1 |
|
|
Substance abuse disorders |
Tobacco use |
13 |
1.3 |
0.73-2.13 |
|
Alcohol abuse |
- |
- |
|
|
|
Total substance abuse disorders |
13 |
1.3 |
0.73-2.13 |
|
|
|
Enuresis |
40 |
3.9 |
2.85-5.21 |
|
Total psychiatric disorders |
120 |
11.6 |
9.76-13.66 |
|
Table 3. Comorbidity of disorders
|
Comorbid disorder
Main disorder |
Mood disorders |
Psychotic disorders |
Anxiety disorders |
Behavioral disorders |
Neuro developmental disorders |
Substance abuse disorders |
Elimination disorders |
|
Mood disorders |
|
0 |
2 (28.6) |
1 (14.3) |
0 |
0 |
0 |
|
Psychotic disorders |
0 |
|
1 (25) |
1 (25) |
0 |
0 |
0 |
|
Anxiety disorders |
2 (3.6) |
1 (1.8) |
|
6 (10.7) |
2 (3.6) |
0 |
8 (14.3) |
|
Behavioral disorders |
1 (3.2) |
1 (3.2) |
6 (19.4) |
|
1 (3.2) |
4 (12.9) |
3 (9.7) |
|
Neurodevelopmental disorders |
0 |
0 |
2 (6.7) |
1 (3.3) |
|
1 (3.3) |
2 (6.7) |
|
Substance abuse disorders |
0 |
0 |
0 |
4 (30.8) |
1 (7.7) |
|
1 (7.7) |
|
Elimination disorders |
0 |
0 |
8 (20) |
3 (7.5) |
2 (5) |
1 (2.5) |
|
Discussion
In this research, we described the epidemiology of psychiatric disorders among children and adolescents that reside in Bushehr Province, at Iranian southern coast with Persian Gulf. Totally, 11.6 percents of children and adolescents in Bushehr were affected by at least one psychiatric disorder. This overall prevalence rate obtained in the study clearly shows that the prevalence of mental disorders in Bushehr is lower than most other provinces in Iran including Tehran, Isfahan, Mashhad and Ardabil. Alavi et al 10 and Khaleghi et al 11 reported a total prevalence of mental disorders of 17.9% and 28.2%, respectively, in children and adolescents living in Tehran. Arman et al 12 revealed that 26% of children and adolescents living in Isfahan had psychiatric problems. Moharreri et al 5 showed that 34% of children and adolescents living in Mashhad had psychiatric problems. In another recent study in Ardabil province, Molavi et al 13 reported a total prevalence of 31.7% in youth population. However, the estimated prevalence in this study is comparable to the findings of Mohammadi et al 6, which was conducted in the five provinces of Iran.
Anxiety disorders were the most prevalent disorders among the children and adolescents of Bushehr, which is similar to the findings of Khaleghi et al. However, most previous studies 5,6,12-16 reported Attention Deficit Hyperactivity Disorder (ADHD) as the most commonly diagnosed disorder in children and adolescents, Which was estimated at only 1.3% in our study. For example, Molavi et al, Alavi et al and Moharreri et al reported a prevalence rate of 12.5, 8.6 and 5.8%, respectively, for ADHD. This difference is probably due to either the socioeconomic differences between the provinces or underestimation of prevalence of ADHD in our study caused by the instruments used and the subjectivity of interviewers. Moreover, anxiety disorders had a high comorbidity with other mental problems. Youth with mood disorders and psychotic disorders were highly vulnerable to anxiety disorders. This observation has also been reported by previous studies 11,17-20. Furthermore, according to the comorbidities results, children and adolescents with behavioral disorders are more vulnerable to substance abuse disorders.
Our results demonstrated that place of residence plays an important role in the mental health profile of Bushehr, so that almost all cases with psychiatric disorders were found in urban areas. This finding is consistent with the results of other epidemiological studies that have been conducted in Tehran 11 as well as other countries such as United States 21, Brazil 22,23 and China 24. It is suggested that serious stimuli and challenges that affect subjects, especially children and adolescents, in large cities may result in a higher prevalence of mental disorders in urban areas than in rural settings 3,21. Meanwhile, the prevalence of mental disorders among girls was higher than that of boys. Also, adolescents (15-18 years old) were more affected by psychiatric disorders than other age groups. These observations are not consistent with the findings of similar studies that have been conducted in Tehran 10,11. This difference can be due to cultural and socioeconomic differences between Bushehr and Tehran. Moreover, our results revealed that low parental education levels may play a role as a risk factor related to the psychiatric disorders in children and adolescents, as previous epidemiological studies in Iran and other countries have been also stated 5,6,25-27. Furthermore, according to the results, parental occupational situations were associated with the mental disorders in children and adolescents.
Conclusion
The estimated prevalence of psychiatric disorders among pediatric population in Bushehr province, justifies particular attention to mental health while making medical policies. The increased rate of disorders in adolescence indicates that screening and early detection of psychopathologies, may diminish the imposed familial, financial and social burden of them. Greater studies concentrated on risk factors, including genetic and familial, social and financial elements can be beneficial in creation of preventive strategies and risk factor oriented screening protocols.
Acknowledgments
Hereby we thank all the families and the children who participated in this survey. We also thank the National Institute for Medical Research Development (NIMAD) (Grant No. 940906), Bushehr University of Medical Sciences and the Psychiatry and Psychology Research Center, Tehran University of Medical Sciences for their financial and non-financial supports.