Document Type : Original article
Introduction
Myofascial Pain Dysfunction Syndrome (MPDS) is a multifactorial syndrome and many predisposing factors as well as risk factors are suggested to be involved in its occurrence 1. Of the orofacial pains, pain of the masticatory muscles is the second most common complaint after toothache 2. Such patients may primarily develop masticatory muscle dysfunction, which is called MPDS 1.
The etiology of Temporomandibular Joint (TMJ) Disorders (TMD) yet requires to be clearly identified; however, the majority of etiologic factors are considered as the predisposing factors 1. Pain in TMJ is a common problem 3. Dentists are the most appropriate health care providers to manage such patients 1. Pain is the most common symptom of TMJ disorders that has physiopathological and psychological aspects 2. According to a conservative estimate, 40-60% of the population suffer from TMD 4 showing its clinical importance. This rate varies from 10-80% in children and adolescents 2. Stress, congenital or developmental anomalies, trauma, ankylosis, neoplasms, arthritis and intra-articular disorders are among the predisposing risk factors that of them, psychological stresses is the commonest risk factor 1.
Muscular insufficiency, psychological conditions such as depression, inflammatory agents and inappropriately high functional loads due to bad habits such as forward bending of the head or shoulders are involved in development of TMD. Clenching when working, bruxism, malocclusion and systemic diseases like rheumatoid arthritis may also play a role. The suggested treatments for these patients include education and rising awareness of causative factors to reduce the effects of risk factors and then physiotherapy, splint therapy, short-term pharmaceutical therapies, fixing parafunctional habits, use of relaxation techniques and use of low level laser 1.
Low Level Laser (LLL) has recently gained attention due to its ease of use and positive analgesic effects 5. LLL does not raise the temperature but changes the structure of the tissue and cells and regulates their metabolism 6. It also stimulates the respiratory cycle of cells 7, increases vascularization and adjusts the orientation of fibroblasts 8,9. Moreover, low level laser can inhibit the activity of some inflammatory mediators leading to pain reduction in muscles and joints, subsequently.
Use of naproxen, which is from Non-Steroidal Anti-Inflammatory Drugs (NSAID) has also been recommended for TMD. I has been observed that the use of 500 mg naproxen had greater efficacy than ibuprofen and Celecoxib in TMD patients 10.
This study aims to compare the efficacy of low power laser and naproxen for treatment of patients with MPDS.
Patients and Methods
This clinical trial with analytical parallel-groups design was conducted on 40 MPDS patients who were selected from all patients referred to occupational medicine clinic of Yazd Province based on standardized examination/diagnosis procedure based upon the Research Diagnostic Criteria (RDC)/TMD. This design was approved by the Ethics Committee of Tehran University of Medical Sciences. Data on age, gender, presence of parafunctional habits, history of facial trauma etc. were collected by clinical examination and a questionnaire. Clinical examinations were done by an oral medicine specialist. Moreover, all patients underwent para-clinical examinations like CBCT.
The exclusion criteria were age below 18 and over 65 years, presence of articular complications, history of treatment for MPDS, systemic diseases and pregnancy 11. Moreover subjects who received analgesic or antidepressant medicine were excluded from the study as well. Patients were randomly divided into 2 groups of 20 cases using foursome blocks and. all of them signed written informed consent forms. The pre-treatment examinations included precise identification of the pain site and determining the intensity of pain were carried out by Visual Analog Scale (VAS), mouth opening measurement using a ruler and assessment of the tenderness of masticatory muscles (temporal, medial pterygoid, lateral pterygoid and masseter) using VAS. Then 40 cases were randomly divided into low level laser and naproxen groups with equal number of 20 patients in each group. Also, patients in LLL group received a placebo drug and patients in naproxen group received placebo laser to eliminate the probable psychological effects of laser treatment. Clinical examiner and statistician were blinded to the group allocation. Group-A patients received 500 mg naproxen (a product of Parsdarou co., Tehran, Iran) every 12 hour for 2 weeks and placebo laser. Group-B patients were exposed to diode He-Ga-Ar laser irradiation (LMPT200, 890 nm wavelength, 10 pulse, E 50 mW power) for 5 minutes for 2 days a week and for 2 weeks plus a placebo drug has been given to them too. Pain intensity, degree of mouth opening in mm and masticatory muscle tenderness were evaluated in patients before and 2 weeks after both types of treatment and recorded in the questionnaires. The amount of mouth opening was assessed by measuring the distance between the upper and lower incisors using a ruler. This distance was measured 2 times and the mean value was calculated and recorded. The amount of mouth opening was measured before and 2 weeks after the treatment.
For the assessment of masticatory muscle tenderness and severity of pain, Visual Analogue Scale (VAS) (0-100) was used. Zero indicated no pain and 100 indicated the most severe imaginable pain. The patients marked on the VAS for 2 times, before and 2 weeks after the treatment and the distance from the marked points to the point zero was measured. The mean of 3 values was calculated and recorded.
Collected data were analyzed using SPSS version 10. Changes in pain, muscular tenderness and the amount of mouth opening were compared using repeated measures ANOVA. Then a p-value of <0.05 was considered as statistically significant.
Results
Of 40 MPDS patients, 20 (50%) were males. Twenty patients were in the laser treatment group and another 20 in the naproxen treated group. The mean age of included subjects was 35.62 (±6.43) years.
Of all patients, 36 (80%) reported no history of trauma to the TMJ while 4 patients had one. The history of bruxism was reported by 5 and clenching by 10 patients. In general the number of patients with parafunctional habit was 27, biting foreign body was 25 and occlusal interference was 1. None of the patients had any systemic disease or drug intake at the time of study.
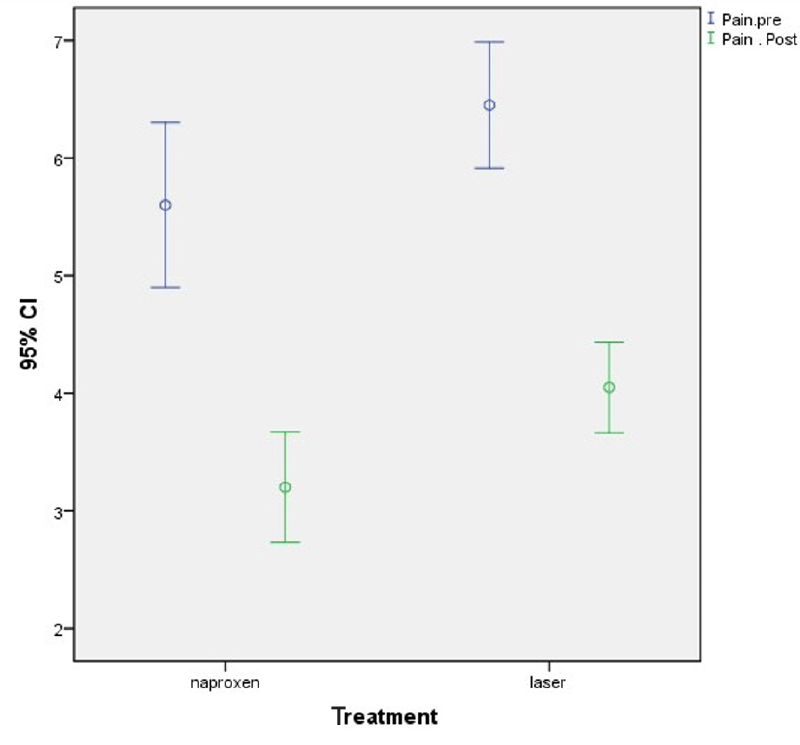
In the naproxen group, the mean pain score was 5.60 before and 3.20 after treatment and in the laser group, they were 6.45 before and 4.05 respectively. Post-treatment pain was not significantly different in either group (Table 1, Diagram 1).
Table 1. Average rate of change in both laser and naproxen pain before and after treatment
|
|
Laser |
Naproxen |
p |
|
Items |
Standard deviation |
|
|
|
Before treatment |
6.45±1.14 |
5.6±1.5 |
p>0.01 |
|
Two weeks after the start of treatment |
4.05±0.82 |
3.2±1.005 |
p=0.01 |
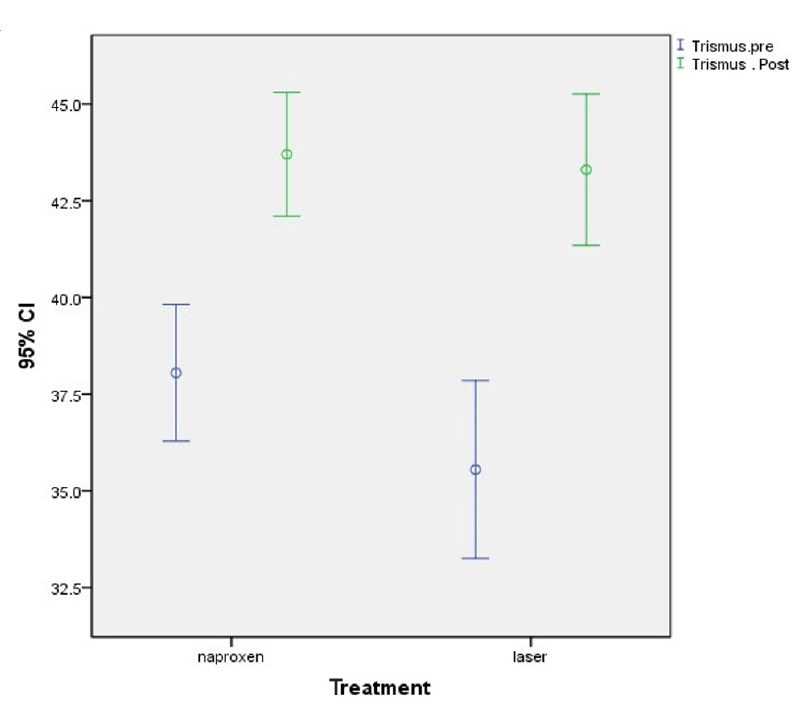
The mean amount of mouth opening in naproxen group was 38.05 mm before treatment and 43.70 mm after treatment (Table 2, Diagram 2) while they were 35.55 mm and 43.30 mm in laser group before and after treatment. Post-treatment mouth opening was significantly different between the two groups (p=0.0007) (Diagram 2).
Table 2. The average laser mouth opening and naproxen groups before and after treatment
|
|
Laser |
Naproxen |
p |
|
Items |
Standard deviation |
|
|
|
Before treatment |
35.55±4.91 |
38.05±3.77 |
p>0.01 |
|
Two weeks after the start of treatment |
43.30±4.18 |
43.70±3.42 |
p=0.0007 |
The mean tenderness of medial pterygoid muscle, temporal muscle, lateral pterygoid muscle and masseter are in table 3.
Table 3. The mean tenderness of the laser and naproxen muscle groups before and after treatment
|
|
|
Laser |
Naproxen |
|
|
Items |
|
Standard deviation |
|
|
|
Temporal muscle |
Before treatment |
6.50±1.39 |
5.35±1.34 |
p=0.20 |
|
Two weeks after the start of treatment |
4.20±0.89 |
3.55±13.09 |
||
|
Masseter muscle |
Before treatment |
6.55±1.23 |
5.25±1.29 |
p=0.15 |
|
Two weeks after the start of treatment |
4.32±0.094 |
3.40±1.09 |
||
|
Lateral pterygoid muscle |
Before treatment |
6.0±1.21 |
5.05±1.23 |
p=0.055 |
|
Two weeks after the start of treatment |
4.20±1.00 |
3.0±1.12 |
||
|
Medial pterygoid muscle |
Before treatment |
6.45±1.05 |
5.20±1.19 |
p=0.17 |
|
Two weeks after the start of treatment |
4.15±0.93 |
3.40±1.09 |
||
Discussion
In this study, the mean age of subjects was 35.62 years old (±6.43). According to the results of the current study and other investigations 12,13 the most common age for onset of this syndrome is between 20-40 years old.
Myofascial pain starts from a trigger zone in a skeletal muscle band. It may occur in any skeletal muscle in the body. Muscles in the head, neck, shoulders and back are the most common site of involvement. According to a study by Peterson, muscular disorder is the most common cause of TMD known as MPDS. The remaining etiologies originate from the TMJ elements themselves 14. In our study, 40 MPDS patients were evaluated consisting of 20 males and 20 females and the amount of mouth opening was measured by a ruler.
In this study, masticatory muscle tenderness was examined using VAS. However Petrucci et al 15 previously evaluated the effect of LLL on the TMJ and Gur et al 16 evaluated the amount of mouth opening in MPDS based on VAS, we separately evaluated each masticatory muscle; which is suggested to be better in comparison with other studies. Kulekcioglu 17 only assessed the amount of mouth opening by a ruler once; while we repeated this measurement for 2 times and the mean value was used, which, as we suggest, would decrease the errors in the mouth opening measurements.
Petrucci et al 15 and Gur et al 16 did not obtain any radiographs of patients, and Shirani et al evaluated the effect of LLL on MPDS patients using panoramic radiography; while in our study all patients underwent Cone Beam Computed Tomography (CBCT); which is more accurate than panoramic radiography due to the fact that CBCT provides a better image of the TMJ and articular disc.
LLLT is a non-invasive, rapid, safe and non-pharmaceutical treatment method that may be beneficial for patients with MPDS but use of naproxen has been recently suggested for the treatment of MPDS. And the number of studies on its efficacy is scarce. In our study, 20 patients received naproxen twice a day every 12 hour for 2 weeks to avoid its probable side effects because administrating naproxen for 6 weeks leads to side effects such as peripheral edema and gastrointestinal complications namely constipation, bloating, stomachache and diarrhea. It should be noted that the therapeutic dosage of naproxen should be administered every 12 hours and must be prescribed for MPDS patients preferably for 10 to 14 days. In another study by Padilla et al 18, naproxen gel was used for treatment and they found no significant difference between the test (naproxen gel) and the control (no treatment) groups; so we used naproxen systemically in our patients (500 mg naproxen tablets). Tablets are also easier to take by the patients while, patients may not comply with gel version of naproxen and it may not be appropriately applied to the respective site also.
We used 890 nm laser irradiation; which resulted in significant pain reduction in our patients, however, in a study by Katsoulis et al 19 they used a 690 nm laser and consequently their laser treated group had less pain than the placebo group; which may be attributed to the low wavelength of laser.
Conclusion
We conclude that due to increasing tissue resistance, laser is superior to other treatments and is recommended for MPDS patients. Also using LLL allows preventing drug side effects which is with better quality of life in TMD patients.
In our study regarding tenderness (pain on palpation) of masticatory muscles and mouth opening there was a significant improvement in both groups but there was not any difference between them. We try to do the best way for comparing these two treatment but we find that the final result was same .It was different with other researches like Khalighi et al 20 that they find better results in using LLL. Ultimately as LLL has less side effect so using laser seems to be better than naproxen
Acknowledgments
The authors would like to thank the Research Deputy of Pardis International University for financially supporting this project.